You know how when you learn a new word, all of a sudden you hear it being used all the time? That’s kind of going on right now with me and hydrogen sulfide SIBO. It kind of feels like everyone I’ve seen lately has suspected or diagnosed hydrogen sulfide SIBO. And it’s funny because before now, it wasn’t that common in my experience.
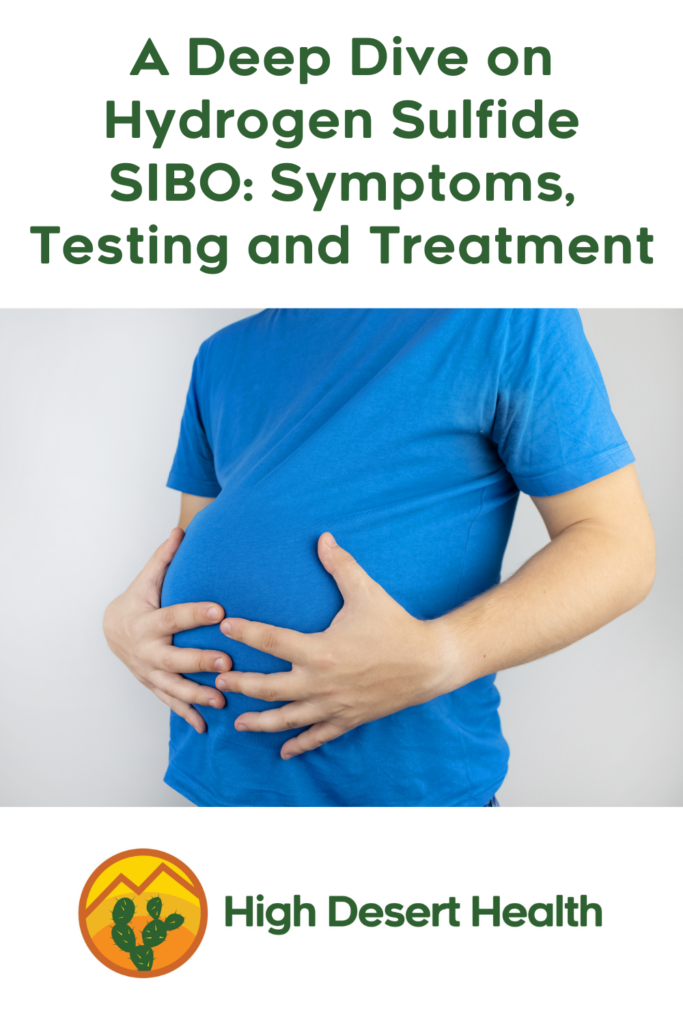
But I’m starting to recognize the type, and if I had to say one thing that tells me that someone might have hydrogen sulfide SIBO, other than a positive breath test or a stool test showing elevated levels of hydrogen sulfide producers or what are called sulfate reducing bacteria, it’s how miserable they are. From a painful, gurgling gut, known as increased visceral sensitivity, to bloating and distension, to excessive burping, to urinary urgency, a burning bladder or interstitial cystitis, to systemic inflammation, rampant food intolerances and often histamine reactions, my hydrogen sulfide clients are just some of the worst suffering. Other symptoms you might see include weight loss, post-prandial hypotension, meaning low blood pressure after meals, weight loss, an elevated heart rate, exercise intolerance, brain fog or insomnia.
Hydrogen sulfide overgrowth is also associated with ulcerative colitis, Crohn’s Disease, colorectal cancer and Parkinson’s Disease, so definitely not something you want to let fester.
And what I’m finding, surprisingly, is that some of my toughest cases of what I though was an overgrowth of methanogens, is in fact an overgrowth of hydrogen sulfide alone or in combination with methanogens. This is because while the overwhelmingly common presentation of hydrogen sulfide is diarrhea or loose stool, it can also present with constipation if there’s an overgrowth in the large intestine or if you have a simultaneous overgrowth of methanogens, which pretty much always causes constipation. The classic example of this is someone with a mixed type IBS where constipation is the usual presentation, but then occasionally there will be bouts of attacks where they have diarrhea and often all-over body pain or extreme abdominal pain, often requiring a trip to the emergency room.
And what a lot of these clients have had in common, if they have constipation, is that they have slowly but surely stopped eating everything besides meat or meat and a limited number of vegetables and maybe a very limited quantity of rice. And they often have histamine intolerance or signs of sulfur intolerance, like the inability to stand cruciferous vegetables or alliums, like onions, garlic, shallots, chives and leaks, which have sulfur. A few have noticed they don’t tolerate red meat, which is particularly high in sulfur. Ironically, all of this may actually stem from a deficit of sulfur, which is a new theory I’m testing out, so I’ll get back to you on that, but this is theorized because of the impact of glyphosate on food, which impairs a pathway in gut microbes called the shikimate pathway. This pathway produces the very important amino acids l-tryptophan, our serotonin precursor, and l-phenylalanine and l-tyrosine, our dopamine precursors, as well as other nutrients. And it’s been shown that glyphosate also impedes sulfur production by causing a deficiency in molybdenum, a cofactor for the enzyme sulfite oxidase, which produces sulfate. Then if you have homozygous copies of the CBS (cystathionine beta-synthase) enzyme, which drives the recycling of sulfur-containing compounds, you may have too much unusable sulfur in your body, which can lead to sensitivities, while simultaneously having a deficiency.
But suffice it to say that hydrogen sulfide is very important in the human body, playing roles in inflammatory, neuromodulatory, immune, endocrine, vascular and respiratory actions. However, at high levels it becomes toxic to cells, inhibiting cytochrome oxidase, a hemeprotein which an important enzyme in the electron transport chain in our mitochondria, which is the way we produce energy in the cells. It also damages the intestinal mucosa and inhibits the oxidation or use of butyrate to feed the colonocytes or cells lining the colon. So upregulating hydrogen sulfide production in the gut may be a compensatory mechanism, but I’ll have to get back to you on my experiments with that.
Which bacteria produce hydrogen sulfide?
So lots of common genuses of gut bacteria produce hydrogen sulfide it turns out, including Escherichia as in E coli, which is not just the pathogenic E coli you’ve heard of, but also includes many commensal species, klebsiella, which is known as the big histamine producer, proteus species and Citrobacter freundii (but not all citrobacters), all of which are part of the family Enterobacteriaceae, some of which are hydrogen sulfide producers. Also the genuses streptococcus and staphylococcus, which I see elevated on virtually every GI Map I see, pseudomonas, H pylori, salmonella, some Clostridium, and Yersinia Enterocolitica. But the two that have been most highlighted as potentially overgrown and relevant to the hydrogen sulfide SIBO picture are Desulfovibrio species and Bilophila wadsworthia.
The interesting thing is that hydrogen sulfide producers come from a number of different phyla, including Deltaproteobacteria, Proteobacteria, Pseudomonadota, Thermodesulfobacteriota, Fusobacteriota and one genus from the phylum Euryarchaeota called Archaeoglubus. And while most are gram negative, one genus, Desulfotomaculum is gram positive and is a spore former. But the majority of the sulfate reducing bacteria are from the genus Desulfovibrio, around 66%, hence why you see those species listed separately on the new version of the GI Map under the heading Commensal Overgrowth Microbes, right above Methanobacteriaceae, the methanogens responsible for intestinal methanogen overgrowth (IMO). And then Bilophila Wadsworthia is in the class Desulfovibrionia and the order Desulfovibrionales but a different genus. And can I just say, bacteria nomenclature is really confusing, even for me? And then finally, Fusobacteria, which is from the phylum Fusobacteriota and the family Fusobacteriaceae, is another one that’s well known to be a problematic one in hydrogen sulfide SIBO, including Fusobacterium nucleatum, known to be responsible for periodontal disease and all sort of other mischief.
What do hydrogen sulfide producers eat?
So the next thing you might want to know about H2S producers is that most of them use hydrogen (H2) as a fuel source, through a process called oxidation. The hydrogen is coming from other gut bacteria that produce hydrogen, which you will certainly be familiar with as the more common type of SIBO. And while hydrogen gas is odorless, hydrogen sulfide gas is smelly like rotten eggs. But again, one of the difficulties in recognizing hydrogen sulfide overgrowth is that many people with it will not say they have gas, smelly gas, or gas that smells like rotten eggs. Or they’ll only occasionally have gas like that, like after they’ve had a meal heavy in animal fat.
But other sulfate reducers use different fuel sources or multiple fuel sources. So for example, Bilophila wadsworthia metabolizes the amino acid taurine. Fusobacterium, Desulfovibrio, E coli and Klebsiella metabolize the amino acids cysteine and methionine. Which makes finding food to eat much more complicated (e.g., protein), but I’ll get to that in a minute.
The other thing you might want to know is that methanogens also use hydrogen as a fuel source. So although you may be negative in a breath test for hydrogen, if you have methanogens and/or hydrogen sulfide producers overgrown, if you kill them off, you may end up with a hydrogen overgrowth. So don’t think that it’s likely to be a one and done program to get rid of these pathogens; sometimes it requires several rounds of treatment with testing in between to see where you are.
How do you test for Hydrogen Sulfide SIBO?
So there is only one breath test out there that tests for all three possible gases in SIBO/IMO, including hydrogen sulfide, and it’s called the triosmart test or order from my Rupa Health Lab Shop*. But stool tests, like the GI Map or GI Effects, can also point to the presence of H2S SIBO in conjunction with symptoms, when you see elevated bacterial markers for H2S producers. You can find all these tests in my Rupa Health Lab Shop*. Although I have been partial to the GI Map in working with clients, I’m beginning to think that the triosmart might make more sense for clients who are constipated, both because you can differentiate between the rarer H2S overgrowth or find out if it’s present alongside IMO, and because then you can track the level of methanogens and determine exactly how bad the overgrowth of methanogens is and have some sense of how long a treatment protocol someone might need. With the GI Map, you’re just seeing stool levels, which isn’t necessarily indicative of small intestine levels. But if you happen to have taken a SIBO breath test that only included hydrogen and methane, the sign that you might have a hydrogen sulfide issue is that you have a flat line or no growth on either of those gases.
I’ve also heard that you can use sulfite urine testing strips* to test for the presence of free sulfites, which may help you diagnose H2S SIBO, but I don’t know the details of how to use the strips in this way.
How do you treat hydrogen sulfide SIBO?
So the bad news for those of you who are on a paleo or carnivore type diet is that the diet for hydrogen sulfide SIBO is actually a plant-based diet. To start with, you want to reduce your animal fat completely, and ideally your animal protein as well, other than fermented dairy, which seems to be helpful in reducing levels of Bilophila wadsworthia, per two studies, one on probiotic yogurt consumption and the other on consumption of a fermented milk product. There may also be benefits for yogurt and kefir consumption in the reduction of Fusobacteria, as an in vitro study found they inhibited its growth. But no animal foods ideally for 3-4 weeks, then you can start reintroducing those foods one by one, starting with the lowest fat types.
But otherwise, you’ll want to decrease fat entirely for 2-3 weeks, definitely avoiding butter and tallow and lard and fatty cuts of meat. Coconut oil and coconut milk in moderation are okay after your initial low fat period. And small amounts of olive oil or omega 3’s are the best choice for fat throughout. MCT oil may also be okay in that initial period and after as it doesn’t require bile for absorption. You also want to avoid simple sugars or high fructose and focus on whole foods with lots of fiber. And then avoid animal protein as much as possible. So basically, you’ll have to incorporate sources of protein that are not animal based, but not including soybeans or quinoa if you have overgrowths of Fusobacterium, Desulfovibrio, E. coli or Klebsiella, as those two foods are high in cysteine. You’ll want to sustain this diet until such time as you are feeling better.
And if the sulfur-containing vegetables like garlic, leeks, onions, scallions, and shallots and cruciferous vegetables bother you, you should limit those as well.
Now if you are one of the unlucky ones who has both a hydrogen sulfide overgrowth and a methane overgrowth and a high level of constipation, you may be asking, what can I eat, especially if that coincides with histamine issues and food intolerances. In those circumstances, I tend to recommend a diet that’s more in between, with a limited quantity of low-fat sources of animal protein like skinless chicken breasts, white fish and shrimp, with low-fat, fermented dairy, nuts, seeds, and any high fiber carbohydrate foods you don’t react to, like lentils, chick peas or beans, starting with small quantities and working your way up, as well as fruits and veggies you can tolerate. Another option of course is doing an elemental diet, which consists of just a liquid diet for 2-3 weeks, which mostly likely you’d want to combine with antimicrobial supplements in order to help it along. I did a podcast on elemental diets, which is episode 100, called Give Your Gut a Break.
This may seem like a scary idea if you have had trouble keeping on weight, but in fact, my guests from that episode, Debbie and Roy Steinbock, maintained that people maintain or gain weight if they have had trouble putting on weight while on the diet. But people wanting to lose weight simultaneously lost weight. So it’s good for any weight circumstances. Or you may just use the elemental diet “shakes” as a supplement to the food you’re eating in order to make sure you’re not losing weight, or to replace 1-2 meals a day. You can find the Physicians Elemental Diet* powder in my Fullscript Dispensary.
What supplements to avoid with hydrogen sulfide SIBO?
So as you’re decreasing sulfur in your diet, you’re also going to want to avoid supplements with sulfur or bile. This includes ox bile, bitters, bile stimulating herbs, carrageenan and additives with sulfur, glucosamine and chondroitin sulfate. You should avoid protein powders with high levels of sulfur amino acids like taurine, cysteine and methionine, although collagen is okay. And then of course avoid NAC (n-acetyl cysteine), glutathione and anything with a -thiol or sulfur group, including alpha lipoic acid. Thiamin or B1 and Biotin also have sulfur, so avoiding high doses of those might be a good idea. Also, certain probiotics are known to produce hydrogen sulfide, so best to avoid those, including Lactobacillus reuteri BR11, Lactobacillus delbeueckii ATC4797 and possibly Bacillus subtilis. There are a couple of others that produce H2S, L plantarum 299v and L rhamnosus GG, but I’ve heard recommendations and studies in which foods or supplements with those strains were helpful in H2S SIBO, so the jury may be out on that.
What supplements are helpful for H2S SIBO?
So what is helpful to take for H2S SIBO? First, there are several herbs that are helpful, including gymnostemma, codonopsis and Korean ginseng, which is panax ginseng*. Then minerals may be deficient that are necessary for repairing bodily processes that aren’t working properly, in particular molybdenum*, 50-150 mcg per dose but no more than 500 mcg/day, or a multi-mineral supplement. I like the Jigsaw Essential Blend Multimineral* as it has zinc, copper, selenium and molybdenum in it at good doses, all of which are recommended for H2S SIBO. Hydroxocobalamin*, a form of B12, is also recommended, as opposed to methylcobalamin, a form I recommend to most clients because of the prevalence of MTHFR SNPs. Then beyond that, butyrate is important (although go easy on it if there’s constipation, only taking one 300-500 mg pill every 3 days if you’re constipated to start). If you’re not constipated, you could use my Tributryin-Max, 1-3 daily, decreasing if you get constipated, or any other tributyrin or CoreBiome based product, although you’ll need more of a lower-dosed butyrate supplement.
Then the prebiotic FOS* is also helpful, 2 grams a day with meals if you don’t react to that. Be careful not to choose one with inulin though as many people with SIBO are reactive to that. And finally, something I’m recommending to most people these days, serum bovine immunoglobulins*, which help bind to and remove gut pathogens without impacting commensal bacteria. The dose that’s been studied is 5 grams a day, which is recommend in two doses of 2.5 grams on an empty stomach, usually first thing in the morning and last thing before bed.
And let me not fail to mention good old Pepto Bismol* or a generic equivalent* or a supplement containing bismuth. MDs will use 500 mg of bismuth three to four times a day with H2S SIBO in addition to Rifaximin, the antibiotic for SIBO. There’s only one product in Fullscript with bismuth that isn’t full of dyes and additives you might want to avoid, which is called Biofilm Phase-2 Advanced*, and has 200 mg of bismuth in two of them, along with some other stuff though that may not be great in H2S SIBO, like alpha lipoic acid. I’m just beginning to experiment with this product, so I’ll let you know how it works out in a subsequent podcast.
And also, I shouldn’t fail to mention that exercise and stress management are also important in managing H2S SIBO.
Well I hope this helps some of you get to the bottom of your gut health or all over body suffering and find a way out.
If you are struggling with bloating, gas, burping, nausea, constipation, diarrhea, soft stool, acid reflux, IBS, IBD, SIBO, candida overgrowth, fatigue or migraines and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me. We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
So I had you on episode five of The Perfect Stool when I was just starting out, where you described doing 9 Do It Yourself fecal transplants on yourself using various donors and your efforts to find the perfect donor and the things that you had done at that point. So I thought this would be a great time to do an update and hear what you’ve been working on. And if you’ve had any changes to your health, so why don’t we start there with your health? And if you can just briefly describe what conditions you would say you had at the last time we spoke and what has changed since then, and how you did it.
Michael Harrop:
Well I’ve had irritable bowel syndrome, chronic fatigue syndrome for most of my life, those are the main things that I’m trying to treat. I can’t remember actually what exactly was different since the last time; there have been like so many different ups and downs. But mild Alzheimer’s symptoms is also something I’m dealing with now, in recent years.
Lindsey:
Like brain fog type of thing, or memory loss?
Michael Harrop:
So there’s actually some really interesting papers on the connection between diabetes and Alzheimer’s. And they call it type three diabetes, I think. And based on the symptoms of what they’re describing, that’s what I have, a mild version of that.
Lindsey:
Do you also have issues with blood sugar regulation?
Michael Harrop:
Not yet that I know of.
Lindsey:
Okay. So, last time, we had talked, you had done nine fecal transplants, have you done more since then?
Michael Harrop:
Yeah, I’ve definitely done more.
Lindsey:
How many are you up to?
Michael Harrop:
I think I’m around like 14 or 15 different donors at this point.
Lindsey:
Okay. Multiple times with single donors?
Michael Harrop:
Yeah, many FMTs from each of those donors.
Lindsey:
Okay. And so did you have any successful ones?
Michael Harrop:
Yeah, I did. I actually pretty much cured my irritable bowel syndrome from one of them. And then I tried another one, which I thought was a 1 in a 100,000 donor. And they turned out to be detrimental for me. And they reversed most of the benefits that I got. And then I continued on with other donors, and I saw continued improvements with them.
Lindsey:
And was your IBS more of an IBS-D type or IBS-C type?
Michael Harrop:
Yeah, it was IBS-C, and then I took an antibiotic called Rifaximin. And it changed to IBS-D. And also I was unable to tolerate proteins and fats.
Lindsey:
That’s a big part of the diet.
Michael Harrop:
Yeah.
Lindsey:
Okay. And now, can you?
Michael Harrop:
So the donor that cured my IBS, they allowed me to reintroduce protein and fat for the first time in a very long time. Other donors were able to restore the fat tolerance, but not the protein so much. At this point, I am still able to tolerate fat, but I haven’t really tried high protein stuff. I don’t have a craving for it.
Lindsey:
So you just eat primarily a diet of what?
Michael Harrop:
My diet right now is, almond milk, malto meal, butter, cheese, fruits, sweet potatoes. Yeah, that’s my diet today.
Lindsey:
Okay, and where did you find the donors that you used?
Michael Harrop:
So in the past, I was just individually trying to find donors. I was going to friends, family, I was passing out flyers at local universities, going online to whatever communities. I was even trying online dating profiles to try to find donors. So I was trying everything I could think of. And eventually, I started up a website called humanmicrobes.org. To officially go into it. And I tried to get the community involved in it at first, because there were hundreds of other people also trying to find a high quality donor. But that didn’t seem too effective. I assumed that people would be enthusiastic about helping and trying to work together to find good donors. But, you know, they didn’t really seem to get involved much.
Lindsey:
Like you wanted other people to help review applications or . . . ?
Michael Harrop:
No, just help spread flyers. Help give advice on how we should go about this, designing of the website and recruiting donors methods and stuff. So when that didn’t work, I decided to try to raise the prices that we were charging recipients and also paying out to donors. And that seemed to be pretty effective. At that point there were only maybe around 25,000 applicants. And then as soon as I raised prices and payouts, we started getting these huge influxes of hundreds of thousands of applicants. And currently, we’re up at almost nearly a million donor applicants.
Lindsey:
Wow, how in the world do you screen that? Do you have some sort of a computer program that helps screen?
Michael Harrop:
Yeah, so thankfully, one of the other IBS patients helped me. They set up a spreadsheet, Excel program that I just input the data into there, and it scores it automatically. So I can score about 10,000 at a time. And that’s really, really helpful.
Lindsey:
Oh, cool.
Michael Harrop:
I wouldn’t have been able to do it without that, I’m sure.
Lindsey:
And so do you feel confident that people are answering questions, honestly?
Michael Harrop:
Yeah, for the most part, people seem to be doing it honestly. But even for the ones that don’t, it’s not really a big concern, because there are other steps that are arguably more important, which is verification of stool type and physical fitness. So even with most people that pass the screening questionnaire, most of them don’t pass the stool and physical fitness verification point.
Lindsey:
So did they send a photo of the stool?
Michael Harrop:
Yeah, we asked for a few days of consecutive samples, along with some physical fitness photos.
Lindsey:
So stool sample photos.
Michael Harrop:
Yeah, right.
Lindsey:
Okay. And then at that point, you’re eliminating them if they’re not fit enough, or they’re stool doesn’t look perfect Bristol, type 3 or 4 kind of thing?
Michael Harrop:
Yeah, so I’m actually looking for some very specific stool type, stool characteristics. It’s more complex than the Bristol stool chart. But that chart is very useful as a basic outline.
Lindsey:
So what does the perfect stool look like to you?
Michael Harrop:
You know, it’s not something that I advertise because I want people to just submit the most accurate photos.
Lindsey:
Okay, fair enough. So how many people have gotten beyond the initial screen, and then the second level of screening?
Michael Harrop:
So about 10 to 20%, pass the questionnaire and go on to the stool and fitness verification. And then from that, I would say, a majority that turn in their submissions either don’t rank high or don’t pass.
Lindsey:
Okay, and how much were you offering to pay donors for each sample?
Michael Harrop:
We are currently offering $500 per sample.
Lindsey:
Okay, and how much are you charging recipients?
Michael Harrop:
$1,000.
Lindsey:
Okay. So, how many people actually have gotten through and qualified as donors?
Michael Harrop:
So we have a list of potential donors that we send out to recipients and recipients get to choose from that list. It kind of depends on supply and demand. I have thousands of possible donors. But right now, there’s only demand for a handful of the very top donors.
Lindsey:
And have they already had their stool sequenced, or what testing are you using after that?
Michael Harrop:
So we’re just using the basic recommended tests, which are just pathogens. The other stool tests, I don’t find them very useful.
Lindsey:
So you’re just doing like, basic GI pathogens plus, are you doing blood testing for infectious diseases and STIs and such?
Michael Harrop:
Yeah, exactly.
Lindsey:
Yeah. Okay. So the donors have to do those at their own expense to be donors and to be on the list?
Michael Harrop:
No, no, we cover all the costs associated with applying to be a donor.
Lindsey:
Oh, okay. So by the time they get through the process, then they have the opportunity to make money but no cost to them to apply. Yeah, that’s correct. Okay. Interesting. And so how many people have you been able to recommend, where there’s been a connection between a donor and a recipient?
Michael Harrop:
Currently, we have three or four donors that have sent out shipments to recipients.
Lindsey:
To how many different recipients?
Michael Harrop:
Well, the two most active ones have sent out to over 100, maybe like one to 200 different recipients?
Lindsey:
Wow. And so are they putting their stool on dry ice? Or what’s the procedure for their stool donation?
Michael Harrop:
Yeah, so they just collect it in a Ziploc bag. And then, depending on what the recipient orders, they’ll then process into capsules, perhaps or maybe an enema solution.
Lindsey:
The donors will do this?
Michael Harrop:
Yeah, we teach the donors how to process their own stool.
Lindsey:
Wow, okay. So the recipients have the option for capsules and the option for . . .
Michael Harrop:
Yeah, recipients can basically choose. We really give a lot of leeway to recipients to customize their orders however they want.
Lindsey:
And for the enemas, are they mixing that with anything or is it just straight stool?
Michael Harrop:
That’s all optional. It’s really up to the recipient. By default we do saline with an antifreeze, either maltodextrin or glycerol.
Lindsey:
Okay. And those are things people can just buy online or where do they get ahold of those things?
Michael Harrop:
Yeah, they’re very easy to obtain. Maltodextrin is a supplement and . . .
Lindsey:
. . . food additive. Yeah. Okay. And what kind of success have you heard about? Do you keep, I assume you keep track of that when you have a recipient?
Michael Harrop:
Yeah, we’re actually the only source of stool donors that’s publicly tracking and reporting results. So anyone can go on our website and see what other recipients have, what results they’ve gotten. Most people I would say, are either getting mild improvements or no improvement. Very few people have adverse events.
Lindsey:
And what are the typical conditions that people are looking for stool donations for?
Michael Harrop:
It’s usually a wide variety of general symptoms. I guess bowel problems are a common one, but not a primary one, I would say.
Lindsey:
Are there a lot of people with say, chronic fatigue looking, or with other sorts of chronic conditions?
Michael Harrop:
Yeah, it’s a wide variety of chronic conditions really.
Lindsey:
Do you have some sort of database or catalog so that you can systematize the responses and analyze them statistically?
Michael Harrop:
I’m not doing any kind of statistical analysis on our results. But since they’re public, anyone is able to analyze them.
Lindsey:
But in terms of the conditions, do you have specific condition lists or specific symptom lists, or are people just describing their own conditions?
Michael Harrop:
Yeah, they’re just describing them however they want.
Lindsey:
Okay. And you mentioned a few adverse events. What kind of adverse events have you seen?
Michael Harrop:
The one I remember is someone just got generally worse. And then I think the worst rating someone gave to a donor was because they got severely constipated. I think those are the only two. They are probably some where they just got generally worse.
Lindsey:
And so you weren’t doing any metagenomic sequencing or anything like that of the stool? So what the contents were of the stool is sort of still a mystery?
Michael Harrop:
Yeah, it’s largely a mystery. But I think for both of our active donors, or the two most active ones, we did the GI Map. And that comes with a few other test results on the gut microbiome makeup, I don’t find it particularly useful.
Lindsey:
Why is that?
Michael Harrop:
Most of those tests are not actionable, and current knowledge is just too limited to do anything with that information. And the information itself is not very useful. It mostly gives information on the genus level or the species level. And there’s just not much you can do with that kind of information.
Lindsey:
What kind of information would you like to see on a stool test that would be more actionable?
Michael Harrop:
I mean, I just don’t think it’s possible with current knowledge, even if you . . . I think Viome might be one that gives the strain info. But even with their tests, and that kind of info, there’s just not really anything you can do with it.
Lindsey:
Because the research is just so early in most strains that are in the gut microbiome?
Michael Harrop:
Right, there’s just no information out there of what you should do, what’s good, what’s bad, because it’s just a very complex ecosystem that interacts together. So maybe you have one strain, if you label it good. But what if it’s not interacting with another strain, then maybe that changes it, and now, it’s bad. So it’s just really complex, and so much is unknown.
Lindsey:
Do you see hope in the future given the rise of Chat GPT and these AI tools for perhaps being able to get further along in integrating the microbiome research?
Michael Harrop:
Yeah, I think AI is the only hope for that.
Lindsey:
Yeah. It’s so complex.
Michael Harrop:
Yeah, there’s too much information for humans to process. It would definitely have to be a computer.
Lindsey:
I’ve done various stool tests over the years. I think I did one, maybe Genova GI Effects with a functional medicine doctor years ago. And then when UBiome was an entity, I did a couple of theirs. And then I did a Thorne, which had meta genomic sequencing. But at some point, I realized . . . oh, and I did one with Biohm. And I realized at one point that there was some 60% that was just not mentioned. And those were the strains that had no name or description. I was like, wait a second, so we don’t actually know what 60% of this is? So we’ve got all these tools in which we’re sure that this thing is a major component of the gut microbiome, it’s super important. But the other 60%, we can’t even identify? So yeah, I guess it is really. . . I mean, I do find some useful things personally, in working with clients on the GI Map, in particular the intestinal health markers, because you can at least see, you know, how’s their output of pancreatic enzymes or their Secretory IgA, so you can get some sense of whether their gut is dysfunctioning and in what way? But yeah, how different microbes interact, and what to do to bring up one microbe, break down another, is still very much only at the beginnings of study for relatively few microbes that are particularly well known. So tell me about what you think about antibiotics and how that relates to people’s gut microbiome?
Michael Harrop:
I think they’re overused, severely. Many of the current studies put it at like 30 to 50% overuse. And that’s according to current guidelines, which I think are way too lenient. So it’s probably way higher than that. And one frustrating way that that’s manifested is that I recently screened a donor that is basically like a one in a million. And they would have had zero lifetime antibiotic use, if not for a week’s use after a dental appointment. And that’s actually one instance, dentistry, where dentists are giving out antibiotics where . . .
Lindsey:
prophylactically . . .
Michael Harrop:
Yeah, it’s not an evidence-based use. They’re just giving it out because . . . I don’t know why.
Lindsey:
Heart murmurs and things like that. I’ve had that before, because I have a super subtle heart murmur. And you’ll only even hear it if I’m lying down. And all of a sudden, I mentioned this, and then I start getting recommendations for prophylactic use of antibiotics. And I’m like, hold your horses. I’ve been having dentist appointments my entire life, and I haven’t had any antibiotics. I don’t intend to start now.
Michael Harrop:
Yeah, I think it even goes beyond that. There were some papers and articles by some reputable websites, where they covered doctors just giving it out where there is no evidence-based use for it at all. So that’s really frustrating to see, especially now that it’s actually interfering with what I’m trying to do with getting super high quality donors that can potentially reverse the effects of antibiotics. Now, this one, the super rare one has been unnecessarily damaged. So that’s kind of frustrating.
Lindsey:
This was somebody who, while you were screening them, had to go and get antibiotics.
Michael Harrop:
No, they got them prior to me screening them. So hopefully, in the future, I can let them know that this is not really an evidence-based use of antibiotics. So you can probably ask your dentist next time, “is this really necessary?” And if you say it is then, what are you basing that on?
Lindsey:
But you don’t allow any donor who’s had antibiotics at all?
Michael Harrop:
I wish I could have a rule like that. But no, that’s so rare to find someone that’s never taken them. So I can’t really impose that.
Lindsey:
Yeah. I think one of my children, I think my older son, but I wouldn’t recommend his stool. But I think my oldest son has never had antibiotics.
Michael Harrop:
That’s nice. Yeah. I think it’s quite strange how there’s this huge anti-vaccine movement, but there’s no anti-antibiotic movement, because the scientific consensus on vaccines seem to seems to be pretty strong in favor of them. However, there’s a pretty strong scientific body of literature showing the harms of antibiotics. So that’s something I find pretty strange.
Lindsey:
I think there is a reasonable anti-antibiotic movement amongst people who are gut microbiome enthusiasts and naturopaths. And that sort of thing. But it’s not anti for any use, of course, because obviously people can die from the infections that antibiotics help them with. I know that for the resistant strains of bacteria, that are resistant to different antibiotics, there’s phage therapy and I have tried to get somebody on here to talk about phage therapy, but that doesn’t seem like a super available alternative to most people.
Michael Harrop:
Yeah, it’s still really early in the research.
Lindsey:
Yeah. So with your donors, the recipients, do you recommend a protocol of a certain number of donations, a certain number of times, antibiotic pretreatment, etc.?
Michael Harrop:
I don’t like to give recommendations because I’m not a doctor. And we try to avoid giving out anything that may be construed as medical advice. But I do have humanmicrobiome.info, which is a website that anyone can use to see what the latest research is on a wide variety of topics related to the gut microbiome. So I recommend that people go there.
Lindsey:
So you keep that separate from Human Microbes just so there’s no conflict?
Michael Harrop:
Yeah, I try to keep them. . .
Lindsey:
. . . liability. Yeah. Okay. Now I know that you have for so many years been documenting research on the microbiome and on fecal transplants, and how do you keep up with all that research?
Michael Harrop:
It’s just like a daily ongoing thing that I’ve been doing for many years.
Lindsey:
And at the time we last spoke, you’d left high school and hadn’t been able to further your education or anything because of your physical issues. Is that still the case? You’re just self-taught on the microbiome and reading science and such?
Michael Harrop:
Yeah, that’s exactly it, yeah. I’m still not able to do much.
Lindsey:
You’re on disability?
Michael Harrop:
Yeah, I’m getting off because I’m making enough money from my business now. But I’m still kind of homebound.
Lindsey:
Right, right. And you look very pale to me. Do you get out in the sun ever?
Michael Harrop:
Exactly. Pretty rarely. Yeah. Oh, actually, one antibiotic I took damaged my skin and made it more susceptible to sun damage. So ever since then, I’ve actually had to avoid the sun more.
Lindsey:
So when we last spoke, I am sure I must have asked you about this. But I’m wondering if anything has changed since. Have you gone through functional medicine testing and providers at all to see if there might be other ways that you can attack your problems?
Michael Harrop:
So in the past, I spent a decade or more just going to whatever doctors I could, and basically they did what they could and I basically learned at the end that they’re really limited in what knowledge and capabilities they have. So it’s up to me to figure out stuff and the gut microbiome may be a solution. But doctors don’t really have very many tools to diagnose and correct a gut microbiome yet.
Lindsey:
And do you take supplements or do things to help your health?
Michael Harrop:
Personally, I’m very limited on the supplements I’m currently taking. I’m just taking zinc and iron, just really basic stuff. I’ve experimented with a lot more supplements in the past. But currently, I’m not really seeing any benefits, any big benefits from most of them.
Lindsey:
Okay. Just curious. So any anecdotes or stories you have from donors or recipients that are worth sharing?
Michael Harrop:
Well, the best result actually came from someone with severe eczema. They said they completely cured it. And we haven’t actually had that many people with eczema or other skin diseases do FMT from our donors. So it’s very possible that we actually currently have a cure for severe skin disorders. But we don’t really know because we don’t have enough recipients trying it.
Lindsey:
Right, interesting. So in your materials online, at Human Microbes, can people find the person with eczema and find the donor and be able to say, I’d like that same donor?
Michael Harrop:
Yeah, they can definitely do that.
Lindsey:
Wow, that’s great. I’ll definitely have to tool around the website and look at that. And we can link to that and then also the HumanMicrobiome.info site. Any other sites that you maintain or have to share info?
Michael Harrop:
Those are the primary ones. Yeah, it’s mostly those two, and I recently set up a forum on the HumanMicrobiome.info website.
Lindsey:
So people can talk to each other?
Michael Harrop:
Exactly.
Lindsey:
Okay. And you also are pretty active on Reddit, right?
Michael Harrop:
Not anymore. Not anymore. And I recommend people avoid that website, actually.
Lindsey:
Oh really, why’s that?
Michael Harrop:
I set up the forum to allow people to get off that website.
Lindsey:
Okay, how come?
Michael Harrop:
They’ve been going on the path of pursuing profit at all costs, and they’ve been degrading their site in that process. And it’s just become a really problematic site in so many ways. I wrote a blog with more info about that.
Lindsey:
So like through advertisements and paid posts, and that kind of thing, or . . .
Michael Harrop:
No. I feel like there’s really nothing trustworthy on that site anymore. It just seems like so much bots, astroturfing.
Lindsey:
What’s that?
Michael Harrop:
Astroturfing is when special interests try to manipulate content in a seemingly organic way.
Lindsey:
Okay, yeah, that’s sort of inevitable in any of these tools, right?
Michael Harrop:
Yeah, but it seems like a big site like Reddit really attracts that type of manipulation. And the Reddit admins don’t really seem interested or able to control manipulation of content on their website.
Lindsey:
So you don’t maintain the microbiome Reddit or . . .
Michael Harrop:
No, I’m pretty much off of Reddit completely right now.
Lindsey:
Okay, you handed it over to somebody else?
Michael Harrop:
Yeah, it’s just being modded and kind of referencing the forum. Let people know that they can go to the forum now.
Lindsey:
Okay, that’s good to know. So what are your plans for the future, personally and professionally?
Michael Harrop:
That’s a big one. So at this point, I’ve really done most of what I can on my own. It would be really helpful to get funding for an AI to allow the whole screening process to go through an AI. It’s very difficult. I can’t really pass on most of the screening to another person. And it’s very difficult for a single person to screen almost a million donor applicants at this point. And an AI might be able to learn new things as well, and probably do a better job than me even at the screening process. So would it be great to get funding for that.
Lindsey:
Are your donors coming from multiple countries? Or where are your current donors?
Michael Harrop:
Most of the donors are coming from viral social media videos. So it’s all over the world. In the past, I tried to reach out specifically to top professional and college athletes. And I did contact a few hundred, and got a few applicants from that, but none of them really ranked high. And currently, I’m trying another attempt to contacting top professional athletes; I would welcome help.
Lindsey:
So if somebody is sending from a different country, that’s got to add up in terms of the costs of mailing, no?
Michael Harrop:
Well, our donors mail directly to recipients. So it doesn’t really matter where in the world you live, it’s pretty much the same no matter where they are.
Lindsey:
I mean, how do they keep the sample viable, for whatever length of time it takes the mail?
Michael Harrop:
Generally, they’ll just store them in their home freezer. But recipients can customize their orders, the donor can store it on dry ice immediately, possibly even other things if the recipient needed.
Lindsey:
So they’re storing it in their freezer, and then putting it in the mail for how long?
Michael Harrop:
We do all shipments via dry ice. And usually they will ship around the world in under five days. So we keep them on dry ice all the time.
Lindsey:
So dry ice holds out that long?
Michael Harrop:
Yeah.
Lindsey:
Okay. But you don’t do the shipping. They ship. You’re saying they ship it directly?
Michael Harrop:
Yeah, our donors ship directly to recipient.
Lindsey:
Right. Okay. Well, this is an amazing service that you’re providing for the world. I know that I, for a long time, was really fixated on fecal transplants and the potential they offered. I think they still are a potential goldmine of cures, but I think we are we are still far away from the point of being able to say, well, this is the exact donor for you, which I think is the complex part, right? Because you have these positive effects from one donor that appears not as good as the next donor, and then you have negative effects from that donor. So that’s the tricky part, right? It’s, well I’m deficient in butyrate producers, I need someone who’s really rich in those or I’m deficient in, you know, some other type of microbe or function.
Michael Harrop:
Yeah, possibly. But so far, from what I’ve seen from both our donors, and just other reports that people are sharing from either their personal donors or other donor sources, it seems like donor quality is more important than donor matching. But of course, donor matching does have some importance. But if we can find a 10 out of 10 donor, then possibly donor matching won’t matter at all. But we don’t really know yet, because I haven’t found a donor of that quality.
Lindsey:
What makes you call a donor, a 10 out of 10, something from the original screening or . . . ?
Michael Harrop:
Yeah, so it’s basically the specific criteria that I’m looking for. It’s mostly actually a very, very specific stool type. And I haven’t really found that yet. One interesting tidbit is that, since we pay so much more than everyone else, like virtually every donor that’s been covered in the news, has applied to Human Microbes. And donors from all major clinics, stool banks and companies, they’ve all applied and the vast majority of them either don’t qualify or don’t rank high. I think that only a single donor ranked in the top tier. And that was actually a surprise for me. There’s one donor that’s kind of famous and they didn’t rank high.
Lindsey:
Has the word gotten out in developing countries where there’s a lot less perhaps use of antibiotics or people who are more isolated from Western diets?
Michael Harrop:
Yeah. That’s an interesting question actually, that a lot of people wonder about. It has a lot of problems going that route. The first problem is developing countries are now overrun with antibiotic overuse, because they can get them over the counter. And then another problem is that even as you go to very secluded tribes like the Hadza, which many researchers are doing, they have pathogens from their environment. So it’s not necessarily a great source of FMT. And even if they were, the logistics would be very difficult. Sure, and actually, one of my recipients has gone to the Hadza personally, and did FMT from them. And from what I recall, he got temporary benefits, which were pretty substantial. But then, his long term results were quite poor. And he thinks it was because of their pathogens. He did some testing when he got home, and he tested positive for a wide variety of pathogens.
Lindsey:
Right, right, which they would otherwise be protected for, perhaps because of who knows what else like? I know a lot of a lot of there’s a lot of theory around worms, that worms are a natural part of the human microbiome and prevent, say, allergic reactions to things and people use helminth worms for treating various conditions.
Michael Harrop:
Yeah, the helminth community is pretty interesting. A lot of people decide to do that. There seems to be more research on FMT, though, then helminths?
Lindsey:
Yeah, I was trying to get somebody on to talk about that as well. But they backed out and disappeared.
Michael Harrop:
Yeah, the recipient who went to the Hadza actually got better results from my donor. And it seems because my donors are generally safer, pathogen free.
Lindsey:
Right, right. Yeah. Well, this is all interesting stuff you’re doing and I’m sure that many people appreciate this access to donors, because otherwise they’re not findable. So thank you for your service to the world.
Michael Harrop:
Yeah, absolutely. And I welcome the participation from organizations, philanthropic organizations, such as the Gates Foundation. I would love it if they would help out. Yeah, I think FMT is actually something that would be right up their alley of what they are trying to pursue. And not a lot of other organizations are pursuing FMT, because there’s not much profit to be made. So hopefully, the Gates Foundation is an organization that doesn’t need to pursue profit. So it seems like something that would be good for them.
Lindsey:
Have you reached out to them?
Michael Harrop:
I looked into it before, and it’s something that you have to apply for funding, I’m not sure that I would qualify for funding, they don’t offer just general help. They offer funding for big projects.
Lindsey:
Yeah, I think they’re pretty large scale.
Michael Harrop:
Yeah, I did reach out on X recently, though.
Lindsey:
Yeah, I think maybe a smaller foundation that’s a little bit more out there about what they’re willing to do. But there’s probably plenty of risks, and they probably would want universities to be involved and the approval of medical boards and all that. So that’s the tricky stuff with funding. But it sounds like though, that you’re getting a decent amount of funding now, just via the donations and the recipients in the project itself.
Michael Harrop:
Well, it’s actually not that much, just like enough for basically one person to get minimum wage. As demand increases, it can increase as well.
Lindsey:
Well, I hope it works out and you find your 10 out of 10 donor and are able to completely recover your health. You look at you look a little better to me than the first time I interviewed you, you sound a little bit stronger. So I hope that’s not just my impression, but the reality.
Michael Harrop:
Yeah, I’m not really sure. There’s so many ups and downs that it’s hard to keep track of, but I do publish my detailed results that other people can look through.
Yeah, I publish them on the forum and then also know that I’m using the Human Microbiome donors; all my results are up there as well.
If you are struggling with bloating, gas, burping, nausea, constipation, diarrhea, soft stool, acid reflux, IBS, IBD, SIBO, candida overgrowth, fatigue or migraines and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me. We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
I’m excited to have you on the podcast. I’d heard about ProLon and the fasting mimicking diet at least a couple years ago. And then when it fell into my sphere of potential podcast guests, I was really excited. So anyway, can you tell us about what a fasting mimicking diet is? And how it’s used currently, clinically, in terms of a general overview of conditions and the duration and frequency?
Dr. Joseph Antoun:
Yeah. So as you know, fasting became very popular in the last seven, eight years. And a lot of what was coming from our research – I lead a company called L-Nutra, that produces the ProLon, but we’re a spinoff from University of Southern California where a lot of the research on fasting started. So there’s now 18 universities doing research on fasting. And what they discovered some 10-12 years ago is that intermittent fasting, doing that for a few hours, or extra hours, or 16, or 18, you know, can help people lose some weight. And there’s a lot of clarifications to do there and how to do it the right way. But the biggest discovery was that if you go longer, you know, how about one day, two days, three days, four days, five days, what happens to the body. And one major discovery, which ended up winning the Nobel Prize in Medicine in 2016, was that when you cross the third day, when you go on a third day of fasting, there’s another layer of benefits that happens in the body, which is cellular rejuvenation. So basically, the first two days of fasting, your buddy has enough glycogen in the muscle, I call those then, the checking account and the bank, when you need money, you go first to them, and then you have enough fat, which is the savings account. And then if you need a little bit more on your credit card, the liver can also some can do some neoglucogenesis.
So the first two days, you go to glycogen and fat and to the liver, and they can help the body sustain. And they when you cross day two, and you’re getting into day three, the body is declaring crisis. It’s saying, well, I’m using my bank account, I’m getting depleted. So it tells the cells that you’re on your own. Now you have to consume the debris, the organelles. You’re going to detox, you’re going to improve how you operate, how you function, otherwise, we’re going to die. So on day two and three, we call this the cellular rejuvenation, and the body is rejuvenating the cells. And if you go long enough, you get to day four and day five, the cells tell the body, hey, I’m using the debris, the organelles, I’m trying to fix and now what’s next. What’s next is there’s some old cells that the body doesn’t need and it kills them, and pushes the new young cells to replace those. So there’s a third layer: the first two days is a metabolic fast, the second, day three, day four, we called it rejuvenation and then as of day four onwards, there’s a regeneration. The body kills the old cells, the senescent cells, which are behind a lot of inflammation and aging in the body, and pushes the young cells to replace them.
Lindsey:
And that’s called autophagy. Right?
Dr. Joseph Antoun:
Autophagy is a second one, the rejuvenation. The regeneration one, which very few people talk about, is all coming from the science of USC and Valter Longo, which he very well described in his Longevity Diet book. If you get anything out of this podcast for those listening to us, go and read The Longevity Diet book, it was an international bestseller. It explains why to go a little bit longer. And what we’re going to talk about it, because we do it to close the question with nutrition. We’re not here recommending that people go and water fast for five days, because it’s so difficult. It’s sometimes risky, and it’s very difficult to comply with. But I’m explaining why we got to the nutritional phase. So the biggest discovery was that two days of fasting, the first two days, is good for your metabolism. Second, day three and day four, cellular rejuvenation and autophagy, Nobel Prize in Medicine. Day four onwards, the way actually that the benefit stays is the body starts killing the old cells, making more structural more deep change and pushing the stem cells, the younger cells to replace the older cells, which is a full regeneration of the body. So it’s a big body detox clean up. And cellular rejuvination makes the body a little bit younger.
That is what made fasting actually very popular is when those cellular changes were discovered. People were like wow, fasting can be a preventative or intervention for many chronic diseases. It can reverse aging, and it can be a very good medical intervention. Medical fasting for people who suffer with from overweight and diabetes, for people with cancer because you starve the cancer, for people with other chronic conditions. And then USC, University of California and the other universities, they went to market trying to tell people to fast for five days and they were trying that with certain conditions, including autoimmune disease and cancer and it was very difficult, nobody was able to do that. But the trials in mice were unbelievable. The cure rate from many chronic conditions. And improving mouse health was very beneficial. So they took the mice data, and they talked to the National Institutes of Health. The NIH funds a lot of research across the US. And they asked for a big grant to develop the fasting mimicking diet, basically, how can we help people eat something during the five days, but mimicking the benefits of fasting on the cells.
So that was the big endeavor, and it took $36 million, actually, of the grants and donations, it took 12 years for those researchers to sit and say, okay, how much of every macro and micro-nutrient can I give you and at what time of the day and combined with which other micronutrients, what we call the nutrient sensing pathways, the cells have receptors to food so that we don’t trigger the receptors of the cell so that the cells do not recognize their eating so that the cells stay in the fasting mode. So it took 12 years, a very precise precision nutrition formula that gives you all plant-based, healthy ingredients, no chemicals, no extra processing, it’s just literally high-end, premium, clean food that is made of ingredients tested to not trigger the satiety of the cell and therefore keeping your body in the fasting mode. Although you’re eating for five days, and this is why they call it the fasting mimicking diet, probably the biggest oxymoron you’ll hear in nutrition, it’s a fasting food basically, much better than fast food, by the way.
Yeah, the way the consumer would see it, and ProLon is the brand name of the fasting mimicking diet. So if you consume ProLon, you’re having a fasting bar in the morning. You can actually buy by the bar separate, it’s called the fasting bar. So you get a bar for breakfast, then you get a soup, and some olives and then supplements for lunch. You have a small snack, that chocolate crisp, in the afternoon. And for dinner, you will have another soup and crackers. And you have a drink that you take throughout the day and your supplements, minerals and an algal oil as well. And it’s all vegan. And this is the presentation level. But the ingredients themselves, the macro ingredients, a lot of them are coming from high end nuts. So you have macadamia, you have almonds, pecans, because they have the right proportions of healthy fats for the brain when you’re fasting. They have the complex carbs; you don’t want to have short carbs, because they spike insulin, they spike the detection of the cells. And they have plant-based sources of proteins, which is very effective for actually maintaining lean body mass.
This is one of the biggest surprises with ProLon is when you do fast and you do it a little bit longer term, you lose a little bit of muscle here and there. But when you do ProLon and there’s two clinical trials on ProLon and patents filed, you protect lean body mass. So what happens is the cells of the muscles are rejuvenating and then what makes fasting different than all other diets, it’s a stress reaction that is induced in the body, it’s why the cells rejuvenate. Whereas any other diet is a calorie deficit. So the body adjusts by losing fat and losing a little bit of muscle. But with fasting it’s a stress, and stress increases stress hormones, one of which is growth hormone. So when you’re doing ProLon, growth hormone is high in the body. And now because you’re doing a fasting mimicking nutrition, you’re getting proteins to the muscle, and we have a secret in it, where we spike the carbs a little bit in the soups, which spikes insulin little bit, without going off fasting. And now the muscle is seeing a mini spike of insulin, it’s seeing a spike in growth hormone because of the stress and it’s getting fed because it’s a nourished fast. So the muscle gets maintained and in many cases, actually increases. So it’s one of the most important features of doing fasting with nutrition versus not. And it’s helping a lot of people when they get off of ProLon to still have high metabolic rate, to still be vibrant, to still exercise, to not pick up the weight right away.
A lot of the metabolic benefits with ProLon last three to four months, so 90 to 100 days after just doing that five days of fasting mimicking nutrition. We’ve tested it against the Mediterranean Diet, against a lot of pills for diabetes, including the Ozempic’s and Wegovy’s and the insulin and the effect is by hundreds of percentages better, mainly because cell rejuvenation, when you’re getting younger, a lot of the chronic diseases we suffer from today are due to aging. So you want to hit on two things. You want to get your body a little bit biologically younger. There is nothing today that you can take that is proven to get you get your cells younger and fixed, except fasting. Right so that’s one of the biggest impacts and people need to understand that 90% of us are dying from four conditions today, right? Cardiovascular, diabetes, cancer and Alzheimer’s. These are not independent diseases. These are not genetically driven. To a certain extent, yes. But these are mainly diseases of aging. Even if you have the APOE gene, if you’re not 70, you’re not going to get Alzheimer’s. You know, most people have diabetes at age 60, they were still a little bit overweight at age 40, and 30. But they did not get diabetes, because they had younger cells, they had better muscle, they were able to deal with excess carbs.
So reversing biological age is key to escaping or preventing or better dealing with these chronic conditions. And this is why we’re seeing the fasting mimicking diet and the clinical trials, we now have over 32 clinical trials and 18 top universities globally, we’re showing major health benefits in chronic conditions because this is the only intervention that is rejuvenating the cells, getting you a little bit younger. A younger you has a much better body and biology and metabolism to deal with conditions. And the second biggest secret is protecting the muscle, the muscle is very important for viability, for burning carbs, for decreasing insulin resistance. And as you know, 73% of us have a certain level of overweight and now the latest statistics are showing that 90% of us have certain metabolic issues. So getting the body younger, protecting the muscle, turns out to be way superior to the Wegovy’s and the Ozempic’s and the chronic dieting. And this is what’s behind the success of ProLon and fasting today.
Lindsey:
That sounds amazing. One big question that hits my mind because when I think of fasting, my biggest fear is hunger pangs. So do you still get the hunger pangs with ProLon?
Dr. Joseph Antoun:
Different people have different experiences. So if we take 100 people, the statistics show that a third will say it was very easy, and I’m used to it. And these are typically people who are metabolically flexible, they exercise or they try to keto, meaning their body easily switches to ketones, easily breaks down fat, easily calls for liver for executing. They flex, they do exercise, they are in general healthy, and sometimes they’ve done some ketogenic diet. So they find it very easy. There is a good 40% that find it, okay, it was challenging, and especially on day three, when now the pressure’s on the cells to rejuvenate, but then they go through it. And there’s a good 20% that say it was very difficult. And these are typically people who are not metabolically flexible. They’ve addicted their body to carbs or others and they find it difficult to jump and do it.
But then every cycle you do it, we show that it becomes easier and easier, because your body now, it’s like exactly when you go to the gym, right? If you’re used to going to the gym, it’ll be easy. If you’re not used to it, the first time, you’re going to have a little bit of muscle ache, and you’re going to feel tired the next day. And we see the same. Fasting is actually like intensive training; it is the same mechanism. It’s the same way they tell you to do intensive training now, and then it opens new vessels for the heart, it takes your body to the next level. It’s just a stress imposed on the body. When you impose a stress, the body elevates its defense mechanism. And a lot of those are great mechanisms for aging, the same way fasting does the same for the cells. At a much more advanced level. Obviously, we talked about rejuvenating yourself. Because you’re going five days, it’s not few hours of stress, it’s a five day process. But over a million boxes now consumed. It’s only five days. Statistics show that 91 to 93% of people would be able to complete it. But again, some people find it difficult the first cycle.
Lindsey:
And so I’m thinking about the fact that obviously somebody who is a bigger man versus a small woman typically consumes a lot different number of calories. Is it in any way calibrated to weight?
Dr. Joseph Antoun:
It’s not and I get this question very frequently. And we tested it on different BMIs. We tested it on different body weights, on different muscle mass, and why we don’t calibrate it is because it actually auto corrects, meaning if you’re a bigger weight, you have a lot more reserves, you will get into autophagy towards day 4 not day 3. Because you have more reserves, you can cope more. And your metabolism is not probably as active as a person who’s skinnier and who has less reserves and has a lot of muscle. And so what happens is, if you’re bigger, you get autophagy on day four. And if you have a higher metabolic rate and you have less fat and your BMI is lower, you get into autophagy towards day 2, but why we don’t want to autocorrect because for the person who has a lot of reserves is you’re going to give him even lower calories to get him into autophagy sooner and the lower calories becomes a risk to that person. Because that person is addicted to the carbs a little bit more and has a bigger volume intake, so it self corrects. And the same way you don’t want to rush an already skinny person who already has a high metabolic rate into autophagy. So what happens? It self corrects and it works for each one, balancing compliance, safety and efficacy together.
Lindsey:
Okay. So let’s talk about the research on the fasting mimicking diet and inflammatory bowel disease or Crohn’s and Colitis.
Dr. Joseph Antoun:
Well, yeah, this is a very current topic. Stanford University is doing a trial on Crohn’s and University of Miami is doing a trial on ulcerative colitis. And we don’t have yet the results published. But what we have studied extensively is in mice first, we studied fasting, water fasting. We studied the fasting mimicking diet, ProLon and we looked at the benefits and in at least in mice, again, I cannot confirm it, in humans until we have the results of the clinical trials, and with compliance we don’t want to over . . . although we have a lot of cases reported to us of a lot of benefits. But I’ll stick to the results in mice. And in mice, what we showed is that water fast doesn’t actually . . . so inflammatory bowel disease, or autoimmunity, and you also mentioned ulcerative colitis, the common factor is inflammation. And some of it is an immune reaction to the gut lining. Some of it is also leaky gut, and we can talk about it; there’s so many root causes to each.
But what fasting is showing, water fasting is helping decrease inflammation across the body. We see that all the time. And why is that so? When you do a water fast, the body cannot spend calories right? So the body tells all the white cells, hey, do not . . . inflammation is replication of white blood cells and secretion of cytokines which increases inflammation, it’s like getting the engine of your heart a little bit heated. And when you fast, if you don’t have gas in the tank, you don’t want to to accelerate and hit the engine, because you’re spending it. The same way every time you fast, we see the body dropping inflammation. Now with water fasting, we haven’t seen a lot of benefits on leaky gut. We did see microbiome changes and we saw some stem cell healing in the gut with the fasting mimicking diet and we’ve published that.
We showed it superior to water fasting; this was one of our biggest surprises. Initially, we thought the fasting mimicking diet will give you a portion of water fasting benefits, but it is actually giving more benefits in many cases because it’s funding the rejuvenation. So it’s something to tell a cell do autophagy and I’m going to going to give you minerals and vitamins, you just go and figure it. And it’s something to tell a stem cell or young cell go replicate, fill in the gap for an older cell, but I’m not going to give you any minerals or any macros, versus with a fasting mimicking diet or ProLon, you’re giving them macronutrients and micronutrients. So you’re funding the correction, it’s the same thing.
So we saw a better closure with leaky gut, we saw better stem cell regeneration, or younger cell replication when you do the fasting mimicking diet in mice with IBD, which was a big surprise to us, actually. And we filed a patent on it and we published an article on it. So in general, if we zoom out, why fasting, if you read all books, for autoimmune disease, including IBD: ulcerative colitis and Crohn’s, even the old old book of medicine had fasting. And why is that, it’s very interesting. So we talked about decreasing the immune attack, because when you fast the body doesn’t want to fund any replication of white blood cells, it doesn’t want to secrete cytokines and increase temperature, but also actually, we see the body killing the active T cells and regenerating new naïve, we call them naive new cells, because they’re not going to do that attack. So it’s part of the body’s human evolution and natural selection of hey, if by mistake I have white blood cells, T cells doing a lot of attacking, let me just wash them out and bring new T cells.
So we see this all the time, immunity and limit drops, and limit increases, showing the regeneration, so very interesting to swap active cells with naive new cells that will not do the attack, but also on the heat on the damaged organ. You know, whether it’s psoriasis, whether it’s rheumatoid arthritis, whether it’s all sort of colitis, we talked about autophagy and cellular regeneration, so we see healing happening at the damaged organ, and this is why fasting has been so effective in autoimmune diseases. It decreases the attack and it helps the damaged organ to heal. And I was just fascinated. I’m a physician myself, but we never learned that. But when I went back and one night I was looking at the old interventions in autoimmunity and fasting was core to those. So now with the fasting mimicking nutrition, we are testing in humans whether we can get the same benefits or maybe it could be better could be not, before we announce officially announce and launch our autoimmune programs.
Lindsey:
You have studied MS though, correct?
Dr. Joseph Antoun:
We have studied MS. In same concept what we’ve seen in MS. We studied in humans and we studied in mice. And in humans, we studied one cycle, followed by the Mediterranean diet. One cycle of fasting mimicking diet, followed by the Mediterranean diet. In MS, the same as other autoimmune systems, you see the immune attack goes down pretty fast in mice, actually 20% of the mice reverse all the immune attack in the first cycle of the fasting mimicking diet, which is striking. And then when you go and we’ve shown on MRIs, the damage, you know myelin around the axons also gets rejuvenated and gets healed. So, again, I cannot confirm all this in humans, were a science company. So we have to do clinical trials. This is why we have 32 clinical trials, we take every condition and we go with it.
Lindsey:
Okay, so only so far you have mice results?
Dr. Joseph Antoun:
We have mice results showing, because this is you know, invasive, we’re showing the rejuvenation in the myelin of course. In humans, we do have an early human trial. It shows symptomatic improvements, but we haven’t done an invasive, big trial on humans to show full rejuvenation happening.
Lindsey:
Okay, and that was with one cycle. There were symptomatic improvements.
Dr. Joseph Antoun:
It was a feasibility study. So typically, when you do mice trials, and you go to human trial, you start with a small trial in humans just to show safety and feasibility. So we’ve done a quick one, we show it’s safe for people with MS to do the fasting mimicking diet, it was ProLon that time. And then we show it’s feasible; at least it’s not making them worse or putting them at risk. Then you go to phase two, phase three, which are the bigger, bigger interventional, bigger volume of fuel. We haven’t done that.
Lindsey:
Okay. So I know that the most recent paper published or at least when we originally spoke was on diabetic nephropathy, and the fasting mimicking diet. Can you tell me about that study?
Dr. Joseph Antoun:
Yeah, and now we just published another one, two days ago. So this is diabetes, we have launched what we call the L-Nutra Health for Diabetes Program or fasting mimicking diet for diabetes program. We’ve done two clinical trials on diabetes. And diabetes, we’re most excited about, number one, because it’s the one of the biggest diseases, so we can help so many people, and hopefully millions of people.
Lindsey:
Type two diabetes?
Dr. Joseph Antoun:
Type two diabetes. We’ve study type one in mice, we’ll talk about that. But yes, type two, and then what we’re excited about also is that diabetes is a actually a combination of four things. And again, I am an MD PhD, but I’ve never been taught these four things behind diabetes. I’ve been taught that blood sugar increases, you give them pills, they’ll take them for the rest of their life, right? I’ve never been taught the true root causes of diabetes and how we can reverse those. So diabetes is, for people listening to us, a pillar of four things. Number one, aging. Again, when you were diagnosed at age 50 with diabetes, you were also eating the same at age 40 and at age 30 and you were a little bit overweight. I’m generalizing, right, most people, or a little bit less weight, but you were younger, your metabolism was higher, and you wouldn’t amass insulin resistance as much as you want to at age 50 or 60 or 70.
Number two, it’s a disease related to muscles. So protecting muscle, and keeping the metabolic rate is very important. It’s a disease of lifestyle, right? And then number four, yes, it is genetic predisposition, but it’s mainly lifestyle as well, and how you eat and how you exercise and stress and sleep. And so the the fasting mimicking nutrition, we’re so excited about it, because it hits on three out of the four pillars. You cannot change genetics yet. But what you can do is you’re helping with the cells getting younger, you’re protecting lean body mass, you lose preferential fat. This is so critical, and I’m repeating myself, but it’s so important, you lose a lot of fat with the fasting mimicking diet. With ProLon you don’t lose muscle, or a tiny bit because glycogen is in the muscle.
And then number three, you’re inspiring the person. A lot of people when you ask about the number one benefit when they finished ProLon or the fasting mimicking diet, they say it changed my relationship with food. And this is a big unlock, because we know that diet and exercise can reverse diabetes if you sustain them for the long term, but it’s very difficult to sustain. And you lose muscle as well when you go on a low calorie diet. But when you do ProLon or the fasting mimicking diet, it’s five days, right? So five days, 90% of people can do anything for five days, right? And then and I always say it’s short enough for people to complete, but it’s long enough to inspire you now to say, wait, is it because when you start ProLon day one you’re like okay, if I’m going to feel hungry on day six, I’m going to have a party. I’m going to eat all the pizzas and burgers. And here comes day four and day five, and he’s like, I just I cannot even see a pizza or a burger. I just want to eat healthy on day six. So that changes the relationship with food, understanding he can go more plant-based, understanding he can eat lower portions, understanding that I don’t have to snack big at night. And I can wait till tomorrow to have my food are very big inspirational steps.
And I’m a big believer in the science coming from Stanford and BJ Fogg about tiny wins, right? So, every time a patient or a person feels like I did something for five days, I think I’ve succeeded, because typically we fail on diets, so they’re chronic. This is a very short diet, right, it’s just five days. I succeeded, I felt that I can go five days on healthy food, why not continue a little bit and then the next cycles reminds you, and then the next cycle reminds you. So it’s very important to inspire people with diabetes to become healthy, rather than just scare them. When they leave the clinic, put them on a very hard diet, and then they just fail, and they learn helplessness, they get acquired helplessness, and they just keep needing more medication and swaping every time muscle with fat. And this is what Ozempic and Wegovy are now doing, accelerating muscle loss and, and we’re waking up now to say, okay, if you stop them, you’re picking up all the fat faster, and you’re not developing the muscle. And this is creating a big issue that we’re facing with these drugs.
So we’re very excited with the fasting mimicking diet for diabetes, because you lose the weight, you protect the muscle, you reverse the bio age, all three big pillars for diabetes remission, we’re seeing a lot of patients in the first clinical trial, two thirds of the patients, reduce medication on month six, meaning they just done it six times, five days, 30 days. So once a month, it’s once a month for six months. And then you maintain just once every three or four months. So very high degree of compliance, that 12 month compliance rate was 83%. Very high chance of reducing medication. This is huge for diabetic patients, because the story for diabetic patients, we start you with metformin, and then we only add, and then you have to inject and then you have to go on insulin, and then you die. This is how diabetes was taught in medical school. And here’s how it’s practiced today versus somebody telling the patient, let’s take you off medication. And so we’re seeing a very high chance of what we call regression, reversing the disease and needing less medication. And a double digit chance of actually remission, which is getting off medication.
Lindsey:
And I assume you’re also tracking hemoglobin A1C and insulin and that kind of thing. What results are you seeing there?
Dr. Joseph Antoun:
Yeah,so within six months, as we mentioned already, a decrease of 1.4 points in HBA1C. And this includes, you know, doctors typically see their patients every three to six months to measure HBA1C, so not only reducing HBA1C, reducing HBA1C on top of taking medication off, because you have to adjust to that effect as well. And so within six months, people on average are dropping 1.4 points of HBA1C, they’re losing 22 pounds on average. 67% are needing less medication at that level.
Lindsey:
And this is with no specific diet in between the five day fasting periods?
Dr. Joseph Antoun:
Zero request to change the diet, zero requests to exercise more. Zero requests to do any changes. We just do the five-days fasting mimicking diet. It’s how we do it with all our trials, otherwise you bias the results and you would not be published in a high-ranking journal or getting any patents on those right?
Lindsey:
Now, I originally asked about diabetic nephropathy and that obviously is different than neuropathy. Can you tell me the difference? And then what you showed in your paper?
Dr. Joseph Antoun:
Nephropathy is the kidneys, neuropathy is nerves, right? And so in that article, we were showing that it’s not only metabolism that you’re improving: blood sugar and HBA1C. But actually transitionally, it wasn’t permanent, but transitionally for patients who tried the fasting mimicking diet that already have diabetes, already have damaged the kidney, because the kidney is the biggest, one of the biggest side effects of diabetes, right. There’s a lot of side effects that happen from diabetes, microvascular. But part of the microvascular is the kidneys start getting damaged. And as you know, a lot of diabetic patients end up with kidney failure and dialysis. We’re trying to see if we can help them temporarily. And we started measuring proteins. Part of the measurement of damaging the kidneys with diabetes is they start leaking albumin. So what we showed is that actually we improve kidney function transitionally in that arc. It was a short term, it was a very short-term intervention. But we saw that after every cycle, we’re showing an improvement in kidney function, which gives us hope to do a longer one.
Lindsey:
Like the eGFR?
Dr. Joseph Antoun:
Yes, and the albumin in the urine, right. So one of the biggest symptoms of damage that diabetes can do.
Lindsey:
Cool. And what is the mechanism of action that the fasting mimicking diet has on diabetes remission and nephropathy?
Dr. Joseph Antoun:
This is what we detail, there’s actually three mechanisms of action right? You lose fat significantly versus protecting lean body mass, number two. Number three is you are rejuvenating the cells, which is very important for metabolism, and then vibrancy of the body to deal with diabetes. And it’s feasible. It’s not a long term diet so people can complete it, patients successfully complete it, and it inspires them to leave a healthier and a better life. All these combined are showing this high effectiveness on the condition.
Lindsey:
Alright, well, let’s talk about type one diabetes, because that is an autoimmune disease. And I do definitely have listeners who are interested in autoimmune disease and have one client who has type one diabetes.
Dr. Joseph Antoun:
And in type one it’s tricky because they are dependent on insulin and you’re fasting them. So it’s always tricky on hypoglycemia. And this is why we haven’t done a human trial yet. And, again, we have stories, but I don’t want to report you successes, because then it will be like as if I’m claiming, and again, we’re a company of science, if anything. If anything, people also want to take from ProLon today, it’s a nutrition product based on science, on NIH money and universities and double blinded, randomized clinical trials, published in top journals. So, I behave the same, we have to be compliant. So I’m not going to recommend anyone with type one diabetes do it today.
But we have seen in mice, because we wanted to test the concept before we go and do it in humans. We’re talking with Harvard University to do the human trial. But we haven’t gotten, we need the funding for it. So we haven’t been able to move forward yet. We’re funding 14 other clinical trials at the same time. But in type one, the theory is the same way we explained it for IBD and Crohn’s and other autoimmune diseases, right. If the premise is that immunity is excited, is attacking the pancreas and the beta cells are not producing insulin, if you fast, are you taking the aggressor, rejuvenating the white blood cells so that you taking the temper and you slow down the aggression, and you give time off for the pancreas to heal and rejuvenate for autophagy and reproducing insulin. So what we’ve done with mice, with a major article in Cell. Cell is the number two science journal in the world after Nature. We have multiple Nature articles, but in Cell, we have seven or eight articles there, we published an article talking about the regeneration of the beta cells of the pancreas, which is the cells that produce insulin. And what we did, we destroyed the pancreas of the mice. And then we put them on cycles of the fasting mimicking diet. And we saw them regenerating beta cells and reproducing insulin and normalizing their blood sugar. It was a huge article for us; it was a big, big achievement. For the first time something describing rebuilding the pancreas and reproducing insulin, it’s amazing. And we’re going to work with the patent on treating diabetes because of that.
But in humans, you have to go and test and maybe in humans, we can reproduce it, maybe not. Or maybe you produce a fraction of it. We have over 15,000 clinics in the US that recommend the fasting mimicking diet. So we have stories, but we cannot base any claim on stories. We have to wait to hopefully find some funding and fund it well, and maybe then be able to help patients either do it or not do it? It’s a tricky one just because these patients are very dependent on insulin and therefore the risk of hypoglycemia with fasting. You’re going to have to do the clinical trial under supervision.
Lindsey:
So back to autoimmunity and IBD. Is there any advice at this point? I know you’re still underway in the human clinical trial. But any advice at this point of how best to implement the fasting mimicking diet in IBD? Like once a month or . . .
Dr. Joseph Antoun:
Yeah, unfortunately, I cannot claim if I don’t have the results. But what I see with some physicians, they do ask these patients to do it once a month. But again, up until I don’t know ‘til when, I don’t know efficacy yet.
Lindsey:
Like when people are flaring or not flaring?
Dr. Joseph Antoun:
Again, this is a tricky question, what answer to help people, but I cannot answer because we sell the product. What I’m going to say is my sister has one, and she does it initially every month and now every three to four months as a maintenance.
Lindsey:
And she has IBD?
Dr. Joseph Antoun:
No, a different autoimmune disease. Again, I don’t want to mention it because I’ll look like I’m claiming . . .
Lindsey:
Right, right, of course . . .
Dr. Joseph Antoun:
Unfortunately. But I can invite you guys listening here to go to your doctor, give him the science. You can go to prolonlife.com (go to https://prolonfmd.com/HighDesertHealth to buy ProLon with Lindsey’s discount). There’s a science section and you can take the articles and then you talk to your doctor. At the end of the day, this is not a chemical, it’s not biotech, it’s vegan five days of healthy food. We’ll have the doctor look at the science and if he decides to supervise you and do it, then it’s his decision but we could not today push that direction.
Lindsey:
Okay, fair enough. So I know that a lot of biohackers use fasting for longevity and such. Has the fasting mimicking diet been compared to water fasting for this application?
Dr. Joseph Antoun:
We talked a little bit about it. Well there’s no randomized clinical trial on water fasting versus the fasting mimicking diet. Nobody has done that. But the goal is again, intermittent fasting is more tested than water fasting. Because there’s no trials where people fast for five days. It’s too difficult. This is why we exist, we actually were a water fasting company, right? And remember, I told you the story and we started at USC, we went into human trials to try it and nobody wanted to fast for 5 days.
Lindsey:
Hard to do you sell that one, though? You can’t make a lot of money off of water fasting, can you?
Dr. Joseph Antoun:
No and it wasn’t a money project at all actually. The founders of ProLon are USC and Professor Valter Longo, again, the author of The Longevity Diet Book, and he donates 100% of his shares to the Create Cures Foundation. I’m happy you mentioned that because this is exactly the opposite of people who found large companies, even in nutrition, and always this device of making money and why our story is always science. And you hear me talking about science and trials, because the founders, they don’t care about the revenues, they actually predonated their shares to the Create Cures Foundation to help patients access new novel innovations.
So we’re sitting on a company that is funded with science, and we have to give back the profits. Yeah, it was a pure need. Actually, this is why the National Institutes of Health stepped in and said, okay, I’m going to give you the funds to create the fasting mimicking diet, because there was no way to get people to water fast for five days. So this is why it exists, right? It exists to help you do a longer fast to reach cellular rejuvenation on day three, we talked about that, versus people can do intermittent fasting on their own 12 hours, and 14 and 16. And you don’t need to always do that with nutrition. Actually, we do have a fasting bar and a fasting shake to do that, because we don’t believe you should starve your body for 18 hours on water, especially when you skip breakfast, because you’re just starving your brain, your heart and your kidneys, the essential organs at their peak performance, which is in the morning.
We’d rather you starve yourself at night rather than you starve yourself in the morning. So we have developed the fasting bar and the fasting shake, just to help people in the morning, consume those as breakfast and then stay in a fasting mode. But we’re less interested in intermittent fasting, it just it helps you with losing weight, it helps if you do it right. With your metabolism, we’re more interested in the longer fast. Again, we don’t recommend anyone do water fasting for a long period. We do it with the prolonged or the fasting mimicking diet. This is why we exist, it was out of the need. And it was to make fasting safe and compliant for most people.
Lindsey:
So this is just a hair off topic, but I have heard people make different claims about when autophagy starts once you start fasting, you know, like how many hours at night to not eat? What is the official word on that? And obviously, it sounds like it differs by body weight.
Dr. Joseph Antoun:
They’re wrong. I used to be politically correct; they’re all wrong. Because it was speculation, right? You know, and I’ll tell you why they’re wrong. Number one is we’re 100% sure they’re wrong. The NIH just deployed eight machines to measure autophagy. So why there’s different theories when autophagy starts, because there was no way to measure it in humans. And now there are eight machines that the National Institutes of Health funded to measure autophagy. One of them is at University of Texas, San Antonio and ProLon was the first product to be tested by the way. And we’re now showing that day one, there’s no autophagy, day two, there’s no autophagy, it’s day three that happens to most people. And so now we have proof and a randomized clinical trial, randomizing people and showing that it happens as on day three. So I can 100% say yes, we got the data last week, so it’s fresh.
But we always knew that. Why because again, the cell rejuvenates. When the when the body tells us, I cannot feed you, you’ve got to go and eat your inside and rejuvenate. And if you skip breakfast in the morning, you still have a lot of fat, you have a lot of glycogen, your liver has a lot of extra reserve, why the cell going to rejuvenate? When you’re not stressed, right? It’s the same way like going into company and telling the CEO, okay, you need a million dollars. I’m going to give you a million dollars but wait for me six hours, he’s just going to wait. He’s not going to go restructure the company. Now if he if you tell him I’m going to come in two weeks, he’s going to be in deep trouble. And he’s going to go and restructure the company and try to fix it and try to save and try to cut. So there’s always a basal rate of autophagy. Every minute of the day, stem cells are rejuvenating just out of normal function and vibrance of the body. But to spike autophagy is definitely not skipping breakfast, not even skipping lunch, not even skipping dinner, you would barely start touching it because it makes sense. You know, you’re not in a stressful mode to go and do it.
Lindsey:
Yeah, so it doesn’t really matter then other than the fact that you’re simply not consuming as many calories that you fast for say 13 hours at night versus 16. Because I know there are some trials on that on intermittent fasting and its impact on blood sugar and all that.
Dr. Joseph Antoun:
Yeah, of course so again, go back to the CEO example. If he needs a million dollars per month, and you’re delaying now for hours, then he has to go and take some money from the banks, the same way, to cover these few hours. Same way the body goes into the fat and breaks a little bit of fat every time you do it. Now, we can talk two hours about that because some people binge eat. So whatever they try to use, they can overabuse after. And it’s very important which time of the day again, we can do a full session on just fasting, a lot of people are doing it wrong, because a lot of the early influencers, told everyone skip breakfast, skip lunch, do OMAD (one meal a day) or do 18 hours. And this is not a longevity practice because you’re basically starving your body in the morning when it needs the calories. And a lot of longevity trials are showing that risk of cardiovascular disease increases if you skip food for a long period during the day and then you binge eat after that. This is what happened.
So why intermittent fasting grew in that sense, because of two wrong pieces of information. They told people they’ll have autophagy if you skip breakfast, which is wrong, and number two, they told them you can lose weight, which is also not always true. And it depends on if you’re eating dinner late. And then you’re skipping breakfast, lunch, and then you’re eating at 4 or 5 pm. What you have just done is you’re stuffing your body and food in the evening time and you go sleep. When you sleep, your insulin and your growth hormone are high at night actually. So you’re in anabolic so you’re storing everything you took in to fat versus and then you go you starve yourself during the day when you need to use these calories for your essential organs. This is a big mismatch. What you want to do, the right intermittent fasting, is you eat your dinner early, and then you stay overnight fasting and then your breakfast, you should get breakfast or get a fast bar or fasting shake. Eat something in the morning because this is when your body needs it. So the right intermittent fasting is 12 to 14 hours max front loaded, sleep on an empty stomach and get your breakfast or delay breakfast. That’s the one that helps longevity. When we study centenarians, people living 100 and beyond, no centenarians do one meal a day or do the crazy starvation stuff. They actually, most of them though, say we eat early, you know, we go to bed early as well.
Lindsey:
Early like five or early like three?
Dr. Joseph Antoun:
Three is an afternoon snack. And honestly, I mean, you can go all the way, the extreme cases. Brian Johnson, he only eats between 8 and 11 in the morning, right. And, you know, we don’t want to go extreme in any way. We believe the best longevity, you get it from harmonization, from harmony, from matching your body with your environment, with the circadian rhythm. This is why intermittent fasting 12 hours overnight works very well, right. So, so what you should do, don’t eat late at night, eat your dinner early, as early as you can wait, and then go to bed on an empty stomach. This is when your body will rejuvenate at night without storing fat. And then the next day you wake up, I always say if you’re sleeping hungry, and you wake up hungry, this is a great longevity practice, and then get your breakfast in the morning. Your brain will be happy because you’re going to work or you have your kids and you need to function. Your muscle is happy because you’re walking, your kidneys are happy, your heart is happy because your heart rate increases when you’re moving. They’re fed on time. And then you go in the afternoon, you eat a little bit or at night and then you sleep and that’s the right practice versus people snacking late at night and then trying to stay 16-18 hours the next day to eat in the afternoon. Your body tells you that you feel weak. You feel the headache, and then you binge eat and then you say I’m not losing a lot of weight and it’s difficult to practice.
Lindsey:
Yeah. It’s a lot more in tune with the European or at least the French way of eating, where the biggest meal of the day is lunch and then dinner is usually just more of a snack.
Dr. Joseph Antoun:
Well, I can give you an advanced trick. How about you do breakfast and dinner and a light lunch like this you would have done two 12 hour fasts. You would have gone overnight to breakfast. And then from breakfast to dinner. That’s another almost intermittent fasting with 12 hours. This is what our founder Professor Valter Longo and again, the Time Top 50 Most Influential People in health care. He’s the number one longevity expert and fasting expert. This is what he does, he eats breakfast, very light snack in the middle of the day to get his body going. And then he eats dinner. Dinner is social. It’s difficult to skip. And so he’s is genius in that sense. He does double twelves in a healthy way rather than staying 18 hours.
Lindsey:
So is he up at five in the morning, I’m just curious, to have an early dinner?
Dr. Joseph Antoun:
No, because you can have your breakfast at eight and then have your dinner at seven. Okay. It’s difficult with work now to eat dinner at five. You’ve got to stay a little bit at work, we’re all really busy. You’re got to be practical. And then you go eat at seven.
Lindsey:
So that’s actually a relatively late dinner.
Dr. Joseph Antoun:
Depends on when you sleep again. But yes seven, in the summer seven, the sun is not down. Early and late depends on circadian rhythm at the end of the day. Because the body follows, I mean, we talked about the Nobel Prize in Medicine 2016 was on autophagy, right? In 2017, it was on the biological clock of the organs. And it follows circadian rhythm. So when the sun is down is the time for dinner. That’s how I say it. And this is why seven is not that late. I mean, winter is 5-6 pm. And in the summer, it’s 7-8 pm.
Lindsey:
But that’s because of daylight savings time and spending time. Right? We altered the clock.
Dr. Joseph Antoun:
No, not the clock.
Lindsey:
Well, okay, that’s true. The sun does naturally . . .
Dr. Joseph Antoun:
Yeah, naturally the position of earth versus the sun.
Lindsey:
But we exaggerated it by adding in daylight savings.
Dr. Joseph Antoun:
One hour in biology is not the end of the day. It’s one hour plus or minus, I’m just saying around that time. You know, having dinner at 5 pm for many people is impossible. They’re still at work. But it should not be at 10 is what we’re trying to say so anywhere from six to seven and eight.
Lindsey:
So you’re telling me my 10 o’clock ice cream snack is not good for me? I at least eat the Keto ice cream or the sugar-free.
Dr. Joseph Antoun:
Yeah, but the calories are being stored. Right. And this is one of the next biggest lies in super, super low carb or low carb, your body lives on carbs. And this keto thing is another podcast that we can talk about. But your body lives on carbs. And if you get the calories from fat and you’re sleeping and you’re in an anabolic state, you’re going to store those. So yeah, definitely don’t go high carb. But you didn’t change much when you eat late at night. It’s the biggest, if you asked me like, and we can talk a lot about what to do to live healthy, long life. But one of the things I always recommend is sleep a little bit hungry. And then everything gets fixed. You’re going to feel like even if you’re eating big breakfast and eating a big lunch, you feel it’s getting burned and you feel you’re going to gain the weight. Sometimes most of us, oh, I don’t eat breakfast. And I’d stay all the way and I only have one meal at night. And I’m not losing that stubborn weight, because you’re eating the calories at the wrong timing. What fasting brought to us is the importance of not just calorie counting, but the timing. During the day you’re catabolic, you’re spending, right, your muscle is moving. During the night you’re storing. Don’t feel the storage, fuel expenditure.
Lindsey:
Right. Okay, well, I think that was a lot of good information that people can use both about the fasting mimicking diet and about just what time of day to eat. So thank you for that. Any final thoughts before we go?
Dr. Joseph Antoun:
No. I appreciate you, Lindsey. I think for those listening here and wanting to enhance the chances of living a healthy, long life, I recommend you do the overnight fast 12 hours, max 14, but just do it in a natural way. Every day there are a lot of people living 100 and beyond who do that. When we study them, eat your dinner a little bit early and stay hungry overnight. You don’t eat overnight, you do two or three times per year the fasting mimicking diet, it’s part of human evolution. This is not our artificial request here. Our ancestors migrated during the winter, they didn’t have food all the time. And they used this time to rejuvenate right? It’s like spring, even in nature. ProLon is like spring; it is when you go and you rejuvenate and then make sure you stress less and sleep better. And then improve your happiness and serenity and social capital. These are the pillars of longevity.
Lindsey:
Awesome. I’ve got links to the various papers in the show notes and to the website to purchase the ProLon, so thank you so much for being with us.
If you are struggling with bloating, gas, burping, nausea, constipation, diarrhea, soft stool, acid reflux, IBS, IBD, SIBO, candida overgrowth, fatigue or migraines and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me. We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
If you’ve been struggling with feeling comfortable in your body, weight gain or weight loss resistance, and wondering if maybe your gut health or gut health issues might have something to do with it, beyond the obvious regarding your diet, I wanted to address that today.
Before I go into that, I should mention that before I focused in on gut health, I worked with clients on sustainable weight loss without dieting, because I think it’s really important that any lifestyle changes you make be sustainable in the long-term. I’m not in favor of, nor do I recommend, low-calorie diets, crash or fad diets, because severely restricting your food intake can disrupt normal bodily functions, doesn’t promote sustainable long-term weight loss and can result in muscle loss and a reduction in your basal metabolic rate, which plays a crucial role in calorie burning. And even worse, undereating often causes your body to store calories as fat. It is not recommended for individuals to consume fewer than 1,200 calories per day unless you’re being supervised by a doctor and I’ve often seen people on such low calorie diets that started to lose weight only when they started eating more.
I also rarely recommend long-term extreme diets like carnivore or ketogenic diets, perhaps with the exception of people who have diagnosed type 2 diabetes that’s in need of immediate and extreme attention. And I think that self-acceptance is very important at whatever size your body naturally rests when you’re eating a healthy diet 95% of the time and exercising regularly, getting good sleep, managing and reducing stress and practicing all of the health-supportive behaviors we all hear so much about. And part of that self-acceptance is consuming media that highlights and supports diverse body types and sizes and reducing exposure to media that exclusively promotes a certain body type or filtered or altered images of unrealistic bodies. And I also think it’s very important, especially if you have any disordered eating behaviors like binge eating, emotional eating, anorexia or bulemia, to address the mental health component of weight gain, especially if you have a high level of Adverse Childhood Events, known as ACEs, that are highly correlated with obesity. If that’s part of your history, I’d recommend looking into trauma-focused therapies, which include modalities like somatic experiencing, AEDP, EMDR and neurotherapy. If you’ve gone through therapy but only traditional CBT-type talk therapy or Cognitive Brain Training, I’d recommend you look into these other modalities in conjunction with whatever other interventions you’re considering.
That being said, research over the last 20+ years into gut bacteria has shed light on its pivotal role in regulating weight and weight loss. So you may have heard about early studies suggesting that a key marker in the microbiome of obese individuals was an excess of gram positive bacteria in the Firmicutes phylum, in particular as it related to gram-negative Bacteroidetes and a high Firmicutes to Bacteroidetes ratio, the two principal phyla of bacteria in the human microbiome. However, these results have been called into question in a resequencing of the DNA from 9 of those previous studies. It was found that methodological differences in sample processing and DNA sequence analysis, interpretive bias and confounding factors that weren’t accounted for such as exercise and altitude, which have been shown to impact the gut microbiota, may have been responsible for these results. Further studies in animals and then in humans over the course of 5 days have shown that the composition of the gut microbiota can change rapidly when subjects are fed different diets. In particular, one study showed that a 5-day animal-based diet increased the abundance of bile-tolerant organisms from the genuses Alistipes, Bilphila and Bacteroides and decreased the level of Firmicutes from the genus Roseburia as well as the species Eubacterium rectale and Ruminococcus bromine, which metabolize dietary plant polysaccharides.
What I believe is a more important factor to consider with regard to weight loss resistance and/or weight gain is lipopolysaccride or LPS, an endotoxin that creates inflammation in the body and is released by and is a component of the cell wall of gram negative bacteria. Studies have shown that elevated blood levels of LPS are associated with prediabetes, diabetes and obesity, while additional studies have shown that translocated gut bacteria are the origin of that LPS. One of the reasons beyond diet that many people end up with elevated levels of gram negative bacteria, in particular from the Proteobacteria phylum, is use of oral antibiotics. As I’ve described in previous podcasts, antibiotics reduce the body’s ability to produce butyrate, the primary food for the cells lining your colon, which comes form the fermentation of fiber in the colon by butyrate-producing bacteria primarily from the Clostridium cluster of the Firmicutes phylum. In animal experiments, 3 days of oral antibiotics decimated the gut’s ability to produce butyrate from fiber and increased oxygen levels in the colon, which is an alternate fuel source for these cells lining the colon. This oxygenation of the colon produces a wonderful habitat for gram negative proteobacteria because they are facultative anaerobes, meaning they can exist in the presence of oxygen. This can then lead to a vicious cycle where proteobacteria continue to dominate, and the colon fails to recover its preferred hypoxic, or oxygen-free state, because of lack of butyrate, and butyrate-producing bacteria that are obligate anaerobes are wiped out. What’s more, a high-sugar diet in rats has been shown to increase proteobacteria, one of the reasons for which I recommend that people eat a super healthy, sugar and flour-free diet while on antibiotics.
The domination of proteobacteria then creates a vicious cycle of high LPS in the body, promoting inflammation, blood sugar dysregulation and increased weight gain. Likely because of this phenomenon, probiotic bacteria that restore the balance of butyrate producers and also mucin-degraders like Akkermansia muciniphila, which reside in the mucous lining of a healthy colon and live in symbiosis with the butyrate producers, have been shown to decrease hemoglobin A1C, a longer-term marker of blood sugar. The first product on the market of this kind, which contains 3 strains of anaerobic, butyrate-producing bacteria, was Pendulum’s Glucose Control*, which has the strains Clostridium butyricum, Clostridium beijerinckii, Anaerobutyricum hallii and Akkermansia muciniphila. While it’s not inexpensive (a monthly supply will run you $177/month via my Fullscript Dispensary, which includes the discount I give my followers), the company’s study on it showed a reduction in hemoglobin A1C of 0.6% and a 32.5% reduction in post-pradial glucose spikes after 12 weeks. You can also get just the Akkermansia* and the Clostridium butyricum* in separate products that are more reasonably priced, which I’ll link to in the show notes.
Because SIBO or small intestine bacterial overgrowth can also cause an overgrowth of proteobacteria, with Klebsiella, Citrobacter and E Coli being three of the most common overgrown bacteria in SIBO, I have also struggled with an overgrowth of proteobacteria, since I have post-infectious IBS which is essentially autoimmune SIBO that keeps recurring because of poor small intestine motility. As a result, I’ve tried Butyricum*, Pendulum’s Clostridium butyricum probiotic, and have found that it is very effective in firming up stool, which is a good indication of butyrate-production in my colon, which slows colon motility. I have found, however, that I can only handle ½ capsule a day, as a full capsule lead to downright constipation and sometimes pain and cramping. At ½ capsule it’s a perfect adjunct for keeping me in steadily perfect stool, along with tributyrin supplementation, the preferred form of butyrate for supplements, which I also have found indispensable in the face of a likely lifelong recurrent Hydrogen SIBO issue.
In addition, direct supplementation with butyrate in various forms has been shown in animal studies to positively affect the function and metabolism of fat tissue, increase insulin sensitivity and help with body weight control. For humans, results have varied between individuals, and I personally only recommend butyrate to people who have loose stool or diarrhea, as it will constipate you unless you use it at very small doses. Its success in weight control in animal studies is likely due to its help in turning around the vicious cycle of proteobacteria dominance in the colon and the subsequent release of LPS. Because of its unpleasant taste and odor as well as absorbability, the preferred forms of butyrate are tributryin, which is what I put in my tributyrin supplement Tributyrin-Max, which is 750 mg a capsule of tributryin, or the CyLoc™ form, an alpha dextrin fiber matrix butyric acid complex, used in Probutyrate*, which is only 300 mg a pill if you want a lower dose, which is more appropriate if you’re starting with firm stool or AuRx*, if you want a powder. Both Probutyrate and AuRx are Tesseract products, and you can find all of these in my Fullscript Dispensary at a discount. If you do have firm but incomplete evacuation or a sense that there’s more to go, I’d recommend starting a low dose butyrate supplement like Probutyrate once every 3 days.
Of course, along with taking probiotics or butyrate, I’d recommend increasing fiber intake through 5-9 servings a day of fresh fruits and vegetables, vegetables primarily, including ½ cup of beans, chick peas, peas or lentils on a daily basis to feed the microbes you’re working to restore in your colon.
Another way in which gut health is connected to weight loss resistance is through low stomach acid. Because sufficient stomach acid is necessary for breaking down proteins into amino acids, if you have low stomach acid, you may become deficient in an amino acid called l-carnitine. L-carnitine is found primarily in animal foods, most abundantly in beef and lamb, as well as formed by the body from the essential amino acids lysine and methionine. Because of this, I often find vegetarians and vegans are deficient in l-carnitine as well. L-carnitine is one of two molecules necessary for bringing fatty acids into the Krebs Cycle for production of ATP or energy. The other is vitamin B2 or riboflavin*. While researching for the podcast, I also happened upon a study that showed that riboflavin supplementation at doses of 50 mg or 100 mg a day also increased butyrate production in the colon, coincidentally. So if you’re struggling with weight loss resistance coupled with low energy (which happens when your fats are being stored and not converted into ATP), and you don’t have a blood sugar dysregulation issue indicated by high fasting glucose or high hemoglobin A1C, you may want to check your fatty acid metabolism through an Organic Acids Test* and/or try supplementing with l-carnitine* or acetyl-l-carnitine* to see if it will spark some weight loss. Typical doses are in the range of 3000 mg/day for l-carnitine when there is a deficiency, some of which can be taken in the form of acetyl-l-carnitine* if you’re also struggling with brain fog or poor memory or other signs of low energy in your brain. And a B complex is often also helpful, so a good quality B complex with appropriate amounts and forms of the various B vitamins is the best choice if you’re trying to cover all your bases with fatty acid metabolism. You’ll be wanting to get at least 50 mg of B2 if you have an identified deficiency.
And then on top of that, you could also start a trial of Betaine HCl*, or supplementary stomach acid, to see if that will help you digest protein better. The usual way is by taking 1 pill with meals with animal protein for a couple days, then moving to 2 pills per meal and up to 5 per meal until you feel reflux, warmth or burning in your chest, then you will want to back down to the previous dose.
Then you should looking at causes for low stomach acid. First, maybe your sodium intake is too low. Salt or sodium chloride, is one component of stomach acid. If you eat no processed foods and salt lightly, you’re likely falling short of the goldilocks levels of sodium, which is between something like 500 and 2300 mg/day, although some sources recommend keeping it under 1500 mg/day. And of course it’s better to choose a high quality salt like himalayan pink salt* or Redmond Real Salt* or one of these good quality salts that have trace minerals rather than just regular store-bought salt.
If you have any signs of gastritis, or inflammation of the lining of the stomach, like gnawing, aching or burning or pain in your stomach (and note that’s different from reflux in your esophagus which can be from low stomach acid), nausea, vomiting, a feeling of fullness in your upper abdomen after eating, trouble with acidic foods, or a known history of H. pylori or ulcers, this can also be at the root of low stomach acid. Healing H pylori, or addressing gastritis first may be necessary as you don’t want to add Betaine HCl or digestive enzymes for that matter, to a stomach that’s already inflamed. You can learn more about that in episode 34 called Upper Digestive Issues.
Next, Candida overgrowth in the gut can also be related to weight gain and weight loss resistance, causing sugar cravings and hormonal imbalances. This can come about from overuse of antibiotics as well as a diet high in sugar and simple carbohydrates. If you have a history of heavy antibiotic use, have a white or yellowish coating on your tongue, crave carbs and sugar, have a history of yeast infections, are usually cold, have fungus in your toenails or have brain fog, these are some of the key symptoms pointing to possible a systemic candida infection. While candida is a normal resident of your gut, an overgrowth of this yeast can lead to systemic candidiasis, where it forms hyphae or tails that poke out holes in between cells lining the intestines, giving it entry into the bloodstream. The only reliable way I’ve found to assess candida in the gut is through an Organic Acids Test. The D-arabinitol marker on the Organix, Metabolomix or NutrEval tests by Genova* is the most studied marker of candida, but I’ve also had good results with the Mosaic (formerly known as Great Plains) Organic Acids Test*, which has a marker called Arabinose. You can get some sense of how systemic and entrenched the candida infection is by how high your level is on these markers. The reference range on Arabinose tops out at 29, and for D-arabinitol it tops out at 36, and I’ve seen clients with results in the 300’s, just to give you some sense of how high it can go, although I’d consider anything in the yellow or red on the Organix or above the reference range on the Mosaic OAT to be treatment-worthy.
To combat candida overgrowth and facilitate weight loss, antifungal herbs and fatty acids are usually needed often for as long as 8 months in more severe cases, along with binders like GI Detox* to catch diet off at first and prevent severe Herxiemer reactions, which is when you feel like you have the flu, as you start killing off bacteria and candida with antimicrobials. And then often I’ll add in a biofilm disruptor into the protocol, often in the second round of antimicrobials. And note that I will typically change antimicrobials for each two-month round in order to prevent any resistance to the products. For a lighter case of candida that’s less symptomatic, serum bovine immunoglobulins might be sufficient to reduce levels. After treating candida, you can restore the gut lining by supplying essential building blocks for mucosal lining repair like glutamine and herbs like DGL, marshmallow root, aloe vera and slippery elm and nutrients like zinc l-carnosine*. I usually add the probiotic S boulardii* as well for candida, as it inhibits candida’s adhesion, morphological transition and virulence. Along with that, I recommend a diet free of added sugar, refined grains, dairy, gluten, yeast, white potatoes and for 2 weeks, fruit, after which time all fruit but bananas are okay. I prefer people follow this diet while on antimicrobials for as long as they can, knowing that realistically if it will take 8 months of antimicrobials, they may not be able to persist the whole time on such a strict diet.
If none of the above work for you, one more drastic method for changing your gut microbiome for weight loss may be through fecal microbiota transplantation, or FMT. FMT is the process of using a healthy stool specimen and transplanting it into the gastrointestinal tract of a recipient for the purpose of improved health. This counteracts the dominance of pathogenic bacteria in the intestines, ideally creating permanent changes to the microbiome. FMT from a healthy donor has demonstrated a remarkable 90% success rate in curing the antibiotic-resistant bacterial disease Clostridium difficile (C. diff), which is a prevalent infection that occurs in hospitals in the United States, affecting over 500,000 Americans annually and causing 14,000 deaths a year. The transplantation of stool from a healthy donor introduces protective bacteria, overwhelming pathogenic bacteria and offering a potential cure for illnesses originating from an unhealthy gut microbiome.
Regarding weight loss, I do have to say that results are mixed and more research is needed to fully understand the relationship between FMT and weight loss. In one study involving 41 patients undergoing bariatric surgery in Finland, researchers investigated the effectiveness of FMT for weight loss. The findings from the clinical trial suggest that FMT did not demonstrate significant benefits for weight loss in patients undergoing bariatric surgery, although its known that bariatric surgery alone changes the microbiome. In this particular study, there were no substantial differences in weight loss outcomes between patients who received FMT from a lean donor and those who received an autologous placebo, meaning they had their own stool put back in. While this study did not find evidence supporting the efficacy of FMT in enhancing weight loss in the context of bariatric surgery, it’s important to note that research in this field is ongoing, and results may vary across studies.
Other studies have shown more promising results. For example, one such study investigated the impact of FMT on weight loss in patients with obesity, considering clinical and microbial factors. The researchers compared mixed-donor nonintensive FMT with single-donor intensive FMT. Results indicated that 13.2% of patients in the mixed-donor group achieved a weight loss of at least 10%, whereas no patients in the individual-donor group reached this threshold. Despite engraftment in all patients, there were no sustained differences between the two groups, suggesting that intensive individual-donor FMT did not induce lasting weight loss or microbiome changes compared to non intensive multi-donor FMT. Notably, mixed-donor FMT led to a durable increase in the abundance and diversity of butyrate-producing bacteria, once again pointing at butyrate as a key player in the question of obesity and the microbiome. The study also identified associations between weight loss and specific microbial changes. Higher initial amounts and reduction after FMT of Bacteroides dorei were linked to overall weight loss, while a weight loss of 10% or more correlated with increased amounts of butyrate-producing bacteria, including Anaerostipes hadrus, Collinsella tanakaei, and Roseburia hominis.
These findings, suggesting differential impacts of FMT regimens on microbial composition and weight loss, highlight the value of personalized microbial-based therapies for obesity based on donor and recipient selection. This personalization could include matching donors with specific microbial profiles to recipients to enhance the success of FMT interventions, although the evidence seems to point more and more to butyrate and butyrate-producing bacteria as a key mover in weight loss. Additionally, the frequency and duration of FMT sessions, as well as associations with specific bacterial species, could be factors influencing the weight loss response. While these findings provide valuable insights, further research is needed to establish broader guidelines for the application of FMT in weight loss interventions.
Another area in which the gut may be affecting weight loss is around gluten sensitivity. One randomized clinical trial aimed to investigate the effects of a gluten-free diet on components of metabolic syndrome. The results indicated that the gluten-free diet led to a significant reduction in waist circumference and improved glycemic control and triglyceride levels compared to the control diet. The findings suggest that a short-term gluten free diet can positively impact some key features of metabolic syndrome, specifically reducing abdominal fat, improving blood glucose levels, and lowering serum triglycerides.
Many individuals without metabolic syndrome may have slight gluten sensitivity, not to be confused with Celiac disease, and this gluten sensitivity could lead to weight gain or hinder weight loss. Leptin, a crucial hormone in signaling feelings of fullness to the brain, plays a key role in regulating hunger and satiety to maintain a healthy body weight. However, individuals classified as overweight or obese often experience leptin resistance. This condition, characterized by high leptin levels without a corresponding cellular response to satiety signals, hinders the body’s ability to manage hunger effectively. A study conducted by Swedish and Danish researchers and published in the December 2005 issue of “BMC Endocrine Disorders” suggests that grains, particularly those containing gluten, may contribute to the development of leptin resistance, potentially leading to weight gain and obesity.
Whatever the mechanism is, I can tell you one thing from my own personal experience. I eliminated gluten because it’s known to be a risk factor for autoimmune disease, and I was trying to reverse my Hashimoto’s thyroiditis. Anyone with an autoimmune disease is recommended to stop eating gluten, because of its role in creating a leaky gut (which also predisposes you to LPS leaking out). As a result of being strictly gluten-free, I avoided so many breads, cookies, cakes, pies, etc. that I would have otherwise eaten, thereby making it much easier to avoid sugar, which of course is related to weight gain. And when I knew I’d be going somewhere with desserts and would feel deprived, I’d make my own almond flour muffins with xylitol as a sugar substitute and eat that instead. And I did, by the way, successfully reverse my Hashimoto’s. I have had normal antibodies for like 3 years now and still have optimal TSH levels and have never had to take thyroid hormones, since my diagnosis in like 2013 or 2014.
So if you’re looking to lose weight, I’d recommend going off gluten, whether or not you have evidence of a sensitivity, because it’s just present in so many processed foods that are so addictive. Or if you want to check whether gluten sensitivity is actually a factor in your weight loss resistance, you can try a short-term elimination for 4 weeks. Without changing anything else, track on a weekly basis your weight, waist measurement at the belly button and any other symptoms from gastrointestinal to skin to headaches, brain fog, etc. and check if you feel better off gluten. If you want to make it super objective, try to replace gluten-based foods with equivalent gluten-free foods, although I wouldn’t recommend breads and desserts and regular pastas for someone trying to lose weight. Be sure to closely check your food, medication, and supplement labels for hidden gluten. Then you can try reintroducing gluten by eating a couple normal sized servings in a day and evaluate your response over the next 3 days.
Finally, I’ll finish up with the more obvious interventions for weight loss but with an eye toward developing and maintaining healthy gut microbiota. You’ll want to incorporate plenty of polyphenols into your diet, which are micronutrients recognized for their antioxidant properties, disease prevention and positive effects on the balance of beneficial gut bacteria. They are found in colorful fruits and vegetables, or products like Poly-Prebiotic powder by Pure Encapsulations*. Great food sources of polyphenols include cocoa powder, berries, dried herbs and spices, hazelnuts, chestnuts, pecans, and red, purple, orange, yellow and dark-green vegetables, as well as beverages like green and black tea. Embracing these polyphenol-rich foods can contribute to a healthier gut microbiome and support weight loss.
Fiber, along with polyphenols, is also recognized as a functional food that provides food for the fermentation of beneficial bacteria in the gut, leading to increased short chain fatty acids like butyrate. Found in undigestible carbohydrates from fruits, vegetables, beans, legumes and nuts, fiber serves as an excellent nourishment source for beneficial bacteria. Gut health is extremely influenced by fiber, evident in the distinctive gut microbiota of individuals consuming animal-based diets versus those favoring plant-based diets. High intake of meat, eggs, and cheeses with low fiber content results in an abnormal gut microbiome characterized by reduced fermentation. Additionally, individuals consuming substantial amounts of animal fat face an elevated risk of pathogenic bacteria, potentially linked to increased iron consumption. In contrast, those with higher intake of plant-based prebiotic fiber from fruits and vegetables exhibit an abundance of healthy bacteria in their guts. Note, however, that this does not apply to ketogenic diets, which bypass the traditional production of butyrate through fiber fermentation and instead produce ketone bodies like acetoacetate and beta-hydroxybutyrate and isobutyrate, a metabolite of protein fermentation, which also help with keeping the lining of the colon hypoxic.
That being said, I am generally a supporter of an unprocessed, omnivorous diet with adequate protein, which is basically one gram per pound of ideal body weight a day, including mostly lean animal proteins, at least 2 servings of fatty fish a week, limited saturated fats but from high quality pastured-raised sources like meat, butter or ghee from organic, pasture-raised animals. Dairy is okay if you have no sensitivity, again from pasture-raised animals, with priority going to fermented dairy like yogurt and kefir and hard cheeses in limited quantities. Then healthy fats from nuts, seeds, avocados and healthy oils like extra virgin olive, avocado, Zero Acre Oil*, which is a fermented oil high in Omega 3’s that tolerates high heat cooking, or flaxseeds or flaxseed oil or walnuts in particular for Omega 3’s if you’re not otherwise supplementing with Omega 3’s or getting them from fish. And then getting a rainbow of fruits and veggies with a minimum of 5 servings a day and preferably as many as 9 servings a day. And then for starches, the best choices are starchy vegetables other than white potatoes, so root veggies, winter squash, sweet potatoes, yams and legumes, quinoa and other whole grains, brown rice, black rice, wild rice or cooked, cooled and either eaten cold or only slightly reheated white potatoes and white rice, which are good sources of resistant starch, which functions like fiber in the body and in particular feeds those butyrate producers.
Generally, to lose weight, most women need to stick to no more than 2, ½ cup servings of these types of starchy foods a day and men may be able to get away with a little more. And if your diet is very far from this, I’d suggest picking one area to tackle each week to move more towards a diet like this so that the changes won’t be overwhelming and will be sustainable.
If you’re looking for help with weight loss, I still work with clients in this area both from the food, mental and lifestyle perspectives through a weekly program that runs for 12 weeks, as well as incorporating testing and interpretation to see what’s going on metabolically that might be impeding weight loss. Or if you are struggling with bloating, gas, burping, nausea, constipation, diarrhea, soft stool, acid reflux, IBS, IBD, SIBO, candida overgrowth, fatigue or migraines and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me. We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
Adapted from episode 110 of The Perfect Stool podcast and edited for readability, with Lindsey Parsons, EdD, Gut Health Coach and Bryce Wylde, DHMHS, ofVennMed in Torontoand co-founder of The DNA Company, who did a DNA sequencing report for Lindsey. To best follow along, download the PDF report.
Lindsey:
Before we launch into my DNA results and what they say about my gut health, can you first tell me about how you arrived at the conclusions that you make in the DNA reports from The DNA Company?
Bryce Wylde:
Well, I had the privilege of under studying with Dr. Mansoor Mohammed, who’s revered probably by most genetic experts, and genomists around the world as within the top 10. So I’ve been in clinical practice over 20 years, and we shared a significant degree of patients between us in this very eclectic multicenter practice called P3 at the time. We no longer practice under the same brick and mortar, but with his IP, and his insights was born a lot of what he would see in this particular DNA report.
Lindsey:
Okay. And this was based on patients that he saw and in their DNA reports?
Bryce Wylde:
Yeah, so Dr. Mohammed had a long standing company and had seen at the time, I believe it was about 2000 individuals, patients of his that he’d done genetic reports on. He has a double PhD from UC Baylor, and was a UC Davis graduate focused in genomic pathways. At that time, along with a team at the DNA company, we amassed another 6000 or so patient samples. Of course, some of this was from his actual clinical experiences, and his former education. From thousands of individuals, we were able to extrapolate a lot of what you now see within the DNA report.
Lindsey:
I think I heard you on another podcast, and you were talking about the fact that there were interviews with patients that was then cross referenced with their genetics.
Bryce Wylde:
You’d have to remind me of exactly what that podcast was, but we certainly would have had a lot of endpoints within any given patient that we consulted with as it pertains to them having gone through genomics. This wouldn’t be exclusively genetics, it would be on all types of functional genomic endpoints and laboratory studies and their full clinical medical histories that would have been taken in combination. Absolutely.
Lindsey:
Okay. I think maybe it was Chris Kresser. Have you been on his podcast? No, I haven’t yet. Okay. It wasn’t Chris Kresser. I can’t remember whose it was then. I’ll have to look it up. So can you explain for people who may order their own reports what the letters mean for each gene. So for example, I show a list of relevant genes under the hormone section. Here’s an example: CYP17A1 and then after that, there’s an AA, and then there’s another one, SRD5A2, and after that, there’s a CG. And then after another one, there’s a CC, and after another one, a CT, and another one, there’s a 2.
Bryce Wylde:
It’s an alphabetical soup. So that’s going back to biology 101, grade 11. Most people that are concerned and are interested in this world of genomics, they’ll often come across the term SNP first or single nucleotide polymorphism. We all have them, they’re not the more revered mutations, but we’ve all started to come to learn to understand and appreciate them. They’re a natural occurrence, a variation of a particular gene, or your SNPs, Single Nucleotide Polymorphism variation. So how your particular gene expresses itself, given some genes are nonsense, or non code, and then others are actually making proteins and hormones and doing other things for us. So out of these important genes that we care to learn about, you have different variations. Some are more common to the population, some are considered to be the preferred variant, while others are considered the poor, or not-so-preferred variant, depending on the context. So when you’re thinking or seeing an A variant, given a particular gene, or an AG, or a GG variant, these variations may be, given that particular gene and whether what it does is optimal, sub-optimal, average, or poor. So it’s kind of like getting a report card, but I should say that there is no perfect combination. No one has the best genes. There’s simply variants that you have and knowing what those variants are can help you get through this game of life. I mean, genes are the cards that mom and dad have dealt you. I like to say that how you play them in this game of life is really what matters. So understanding what those cards are, is akin to understanding what variations or the numbers or letters that add up and how they pertain to your SNPs. So at the DNA company we go further than just looking at SNPs and the conglomerate of variations of those SNPs, we look at pathways. Inclusive within those pathways, often we’re looking at copy number variation. So to your question around numbers, these are like instruction manuals. We’ll talk about this a little bit later on as it pertains to detoxification, for example, the glutathionization pathway. So how our bodies manufacture glutathione and its detox process, you’re getting a whole manual of instruction on how to do that from mom, and from dad. Unfortunately, in some cases, we end up with only one or in many instances, zero copy number variations, or no variant. And then there’s the case of inserts and deletions, whole lines of code. So maybe not the entire instruction manual is missing, but sentences are missing within paragraphs. They’re just not there. Or in some cases, double sentences, so that’s two sentences being redundant. These are known as indels, or inserts and deletions. So we’re looking at SNPs with the AA, AG, GG variation, which one do you have. We’re looking at inserts and deletions, and we’re looking at copy number variations, and putting them all together. You can never take one gene out of context, I like to always add that. You have to consider numerous genes, in many cases, dozens of genes together before drawing even remotest of conclusions.
Lindsey:
Interesting. So when I look at this gene and the letters after it, I don’t know what the default preferred variant is for CYP17A1. I have AA, but I don’t really know if AA is good or bad.
Bryce Wylde:
Well, it’s good, let me tell you, but again that’s taking one gene out of context and looking at it on its own, because it depends on what we’re trying to accomplish in that instance. When we get to hormones, and we certainly will, we’ll cover that that. When we’re talking about the hormone pathway, most folks don’t understand that whether you’re male or female, which is decided by the XX or XY chromosomes, we all produce hormones with the exact same cascade. So look forward to talking about that. With the gene you described, it’s really more specific to how fast you might actually produce estrogen from progesterone. I mean, we’ll get into it. And it’s a really interesting pathway.
Lindsey:
I didn’t want to get to the details of that yet. My comment was more about understanding that as I look at the report, and I see those letters, there’s nothing to tell me right off the bat whether what I have is the preferred or not preferred variant, correct?
Bryce Wylde:
That’s because you’ve got to take them all together. You really look at this as a big book on you. This is your instruction manual. And there’s no such thing as good or bad, really. In instances where we reflect back to or refer back to the literature, and we look at these individual genes as optimal variants, or sub optimal variants, based on population dynamics, it’s very interesting. In some instances where someone has what might be considered the perfect gene, two of them might actually not only cancel each other out, but maybe create a suboptimal combination. So you have to take them all in context, considering where you live, your ethnicity, and your environment, all these things.
Lindsey:
One other question related to that. So if I see two, that means I have two copies of that gene, correct?
Bryce Wylde:
That would be correct. In this instance, we’re looking at copy number variations, or CNV, specific to glutathione, and glucuronidation. The specific ones we’ll be focusing on today are the pathways that are responsible for both detoxification and hormones.
Lindsey:
Let’s start with the detox pathways. How do they relate to gut health? And what does my DNA report say about mine?
Bryce Wylde:
Well, let’s just look. When we put all of these together, and we look at one full and complete list, it’s many pages long, so we’re going to take a minute just to get down to the very bottom of this. Just to summarize, one of our primary focuses being how do you intracellularly produce glutathione. Glutathionization is one of the most important antioxidants, if not the most important. Remember, I was telling you at the top, off-camera, that we don’t actually list a specific detoxification sub report. Detoxification is on page 10 of your hormonal report (p. 144 of PDF), since we’re going to come back to this momentarily. And so what we’re looking at in this instance is, as I mentioned, glutathionisation, GSTT1, or glutathionized theta. Before I get into the depth of your particular findings, you would probably agree with me that elimination of toxins, the liver-gut axis, the microbiome interaction, and the barrier function all play a role, and of course the gut plays a vital role in eliminating toxins and waste products. And efficient detoxification ensures that harmful substances are promptly removed from the system, safeguarding gut lining integrity. GST plays a huge role when it comes to the liver-gut axis. That’s the primary detoxification organ, and its function is very closely linked to gut health. Bile, produced by the liver, aids in digestion and carries waste products and toxins for elimination through the gut. This is also very much involved in microbiome interactions, so it can influence detoxification. Conversely, if you’re not able to rid yourself of toxins and metabolites, this influences the composition and function of the gut microbiome. This is good news for you: we see the number two here next to yours, GSTT1. I shouldn’t forget to mention barrier, so efficient detoxification eliminates the interaction or inflammation between the barrier and maintaining that gut barrier essentially prevents leaky gut, and even leakage of toxins into the system and substrates into the bloodstream. So GSTT1 is supposed to have a copy from mom, and a copy from dad, you got two, so you’re lucky, this is excellent. This is associated, as our report says here, with an increased enzyme function clearance of substrates. So that’s good. We’re also looking at how many GSTM1 or mu 1 copies you have now. This is the master gene that GSTT1, let’s call the GSTM1 a very close, but important, second. You’re supposed to also have a copy from mom and dad, which you also have, which is amazing. Therefore, relating to clearance and processing of xenobiotics and pharmaceuticals and reactive oxygen species, you’re doing very well. So in fact, you are gene blessed, as it relates to glutathionization. GSTP1 is a good example of some variation in a SNP or the Single Nucleotide Polymorphism that sits on this gene RS1695. This is where things may get backed up slightly with you. G variations in individuals we know relate to the ultimate clearance of some things like Tylenol. So that might get a little bit held up. Certain aspects of environmental xenobiotics, those that impact us as it pertains to hormone mimickers, and so forth. This gene, it’s a member, obviously, of the glutathione S-transferase gene family. But looking at this as a single phase two detoxification SNP you are a little more susceptible to certain things, certain health concerns that are associated with toxins, chemicals and certain heavy metal exposure and gut permeability. While there’s no direct evidence linking GSTP1 to gut hyperpermeability, we know that oxidative stress is known to influence the integrity of the gut barrier, obviously. And so it’s very likely that GSTP1 through that role in mitigating oxidative stress might very much influence gut permeability. Superoxide dismutase is very important, as we know, a manganese-driven enzyme and gene. Again, here we’re looking at a SNP, and yours being a CT variation. There’s this association of a 30 to 40% reduction of superoxide dismutase. When we’re seeing the essentially reduced clearance through the GSTP1 and superoxide dismutase, there’s that increased risk of reactive oxygen species accumulating. So you’re going to be interested in managing antioxidants. One of my favorites is the tocotrienols. I’ve done a lot of deep dive into this. Forgive me Lindsey, I’ve seen your whole report, so it’s hard for me to hold back. There’s some instances where we’re talking about gut health, we just mentioned the linkage to liver and that interconnectivity, but because I know about an aspect of your cardiovascular health related to the 9P21 gene. We look at three different SNP variants of that gene and anywhere there’s a G, it’s considered an elevated risk. What we’re talking about with this gene is the potential of inflammation to the endothelial lining. As we’ve known for a long time, the recommendation in this case is to suggest even something like tocotrienols is manyfold. This endothelial lining inflammation predisposition that you have signals to me appropriate consideration for tocotrienols, so not just because of SOD, you’ve got the CT, and GSTT1, you’ve got also the hybrid AG variant, which tocotrienols do a great job of eliminating or sweeping up the mess. This was the work by the way, Dr. Chandan K. Sen of Ohio State University who’s projects get funded $25 million year over year by the NIH, so we know there’s something to them. There’s really great work done there. They looked at post-MI, post-stroke, revascularization and recovery, and white matter lesion reversal. So it’s really amazing stuff. I’ve been to Malaysia, by the way, and I’m not speaking on behalf of the tocotrienols that might come out of Africa or Indonesia, because I’ve never been there. But I hear very terrible things about deforestation. Anyways, tocotrienols from Malaysian Sustainable Palm Oil might be the indication here for you, because of the 9P21 variation and the predisposition to your endothelial lining, and also how it might actually do a great job managing the very slight Achilles heel within your own detox pathways. By the way, the research shows tocotrienols have an amazing capability to reverse NAFLD or non alcoholic fatty liver disease. So there are a lot of little nuggets there to take away.
Lindsey:
Yeah, let me interrupt you for a second because I actually had Dr. Barrie Tan on the podcast, who discovered a source of annatto-tocotrienols. And we talked all about that, and I have subsequently suggested that for a lot of my clients, and I think I have my parents on them and my fiancé on them.
Bryce Wylde:
Well, we’re on the same page then. He has an incredible product that he talks about. The annatto derivative is perfectly good. It doesn’t have to be the Malaysian Sustainable Palm Oil. But the tocotrienols themselves are an incredible antioxidant. So it sounds like we both agree.
Lindsey:
Just so people understand what we’re talking about, we should clarify this is a form of vitamin E.
Bryce Wylde:
Correct. Thank you. And then GPX, glutathione peroxidase. . . . . . of that report. You’re going to scroll down until you hit the hormone report, and then it’s page 12 of the hormone report. We see GPX, and your variation here is a CC. First of all, this gene provides instructions for making the glutathione peroxidase enzyme, so that plays a very crucial role in protecting the body as well from oxidative stress. You’re doing well here. It basically takes hydrogen peroxide and other harmful peroxides in the body, turns them into a very benign and neutral water molecule. Here’s where I just took a quick peek as I scroll down to the end of page 12 and reminded myself of this 9P21 and the fact that you’ve got this between 4 and 6G association. Again, this is the endothelial lining, so this is all relevant within the context of hormones. We stop the detox conglomerate when we go through the GSTT1, GSTM1. You’re doing amazing there with both copies from both parents. On the other hand, GSTP1 and SOD2 are where we want to tweak things a little bit for you, and manage your clearance from phase 2 and just get this sweated out, pee it out, poop it out, get it out. If I’m talking to a client that has this variation combination, if they can afford it, obviously, I often recommend infrared saunas. It’s amazing. Your gut is like inverted skin, and so getting that skin active and sweating out certain things is really good for it. Especially studies show with heavy metals we might do a better job getting rid of them through our sweat pores than we do through our kidney clearance. So that would be the detoxification report in a nutshell.
Lindsey:
We’re on page 12 now (p. 148 of the PDF) Well, let’s move on to methylation. So I’m sure many people have heard about MTHFR. I know there’s a lot of confusion about what that means and how important it is, and maybe some exaggeration of its importance, as well as ignorance about other genes that play into methylation. Let’s dig into that.
Bryce Wylde:
I’m going to go back up a bit here to immunity. And I apologize for flipping all over the place here, but soon I’ll give you the page number within the immunity report.
Lindsey:
All right, and just note that the page numbers restart with each report. So the first one was within the hormones section, pages 10 through 12. And now we’re going to be inside the immunity section.
Bryce Wylde:
Going back to our earlier conversation, a lot of these genes and genetic genomic pathways, you will see some repetition. It won’t be exclusively in the hormone report that you’ll see detoxification, rather it’ll be scattered throughout all the reports. It’s also very relevant to cardiovascular health and disease. It’s very relevant to the hormone clearance that we just looked at. Let’s focus for now on the cardiovascular support. So rather than scrolling all the way up to immunity, because both immunity and cardiovascular involve methylation. Methylation is almost sort of synonymous with inflammation, but not quite. Without oversimplifying, because it is quite a delicate biochemical dance, I look at it like it’s a relay race, where in this race, you’ve got five racers and the baton stands for the methyl group, and the methyl group is CH3. If any of your racers obviously dropped the baton, that’s a problem. It’s not a problem that’s very easily solved by throwing more batons at the race. You’re disqualified if you drop the baton, but it’s of no use to just lay three or four batons on somebody, because more is not always better. So it’s a careful dance, these methylation, biochemical pathway circles. The endgame here for us is to understand what type of support you might need. Through the use of very specific types isomers of B12 and folic acid, we may support and fuel this particular pathway, given the various SNP associations that you might have. As they pertain to gut health, particularly, cellular health is huge, and our guts turn over at a very rapid pace. The immune function plays a role here. As does the microbiome that we already alluded to, in respect to detoxification. As it relates to cellular health, just for example, the methylation pathway and optimal methylation needs an availability of B12 and folic acid. They are imperative for maintaining the health and for repairing the gut lining with that speed of turnover. Obviously, for nutrient absorption, macro and micronutrient, and barrier function are important. When it comes to immune function, methylation plays a very important role in regulating the immune system at large, but it’s also crucial for managing gut health and preventing conditions like IBD, inflammatory bowel disease and leaky gut. The microbiome is a two-way street, but B12 status influences the composition of the microbiome and it plays a role in producing some of it. It also significantly impacts overall gut health in this dance with B12.
Lindsey:
We’re on page nine of cardiovascular report.
Bryce Wylde:
So MTHFR, or methyl tetrahydrofolate reductase. We’re looking at the SNP variant you have here being a CT. I don’t want to get overly complicated here, but this is the one people focus on most often. Sometime the single gene is presented to them, and they think this is the end all and be all even though it absolutely isn’t. I want to remind folks of that analogy I said before. It’s a race. It’s a circular race around the track. They’re really racers. MTHFR is just one of the racers, and it’s a really important racer. It’s part of the pathway catalyzing specifically the conversion of the 5,10-Methylenetetrahydrofolate to the active folates. This 5MTHF is then utilized as a methyl donor to B12 for the conversion of homocysteine to methionine. Homocysteine to methionine, this is the job that this is doing. In you, it’s associated with CT variant to a 30 to 35% reduction of enzyme activity with the intermediate 5MTHF production. We’re not just reporting on this saying that there might be a little bit of an issue here. I’m going to tell you at the end of this, what kinds of B12 and folate are the right ones for you. Because as I was alluding to, just throwing more batons at your racers is not the solution here. That’s called hypermethylating, that can be a problem as well. A lot of folks when they came to learn that they might have a CT or a TT as you do, just throwing extra folic acid at it may not be not only the right solution, you can also throw the wrong kind of folic acid at some some folks, depending on genes within the methylation pathway that are nonspecific to the variations of the MTHFR gene. You wouldn’t know what kind of folic acid to consume unless you went on in this report. Low blood folate is associated with elevated homocysteine levels and increased risk of cardiovascular disease. It’s relevant to you because of the 9P21 gene, and some others. We’ll talk about the maybe the APOE factor. We know all about early pregnancy and normal fetal development. The speed and turnover of the endothelial lining is important to manage. Folate serves as an ingredient to manage DNA turnover. You have this association of 30 to 35% of this enzyme activity and as folate’s crucial for synthesis and repair. And you know it’s vital in maintaining the health of these rapidly dividing cells in the gut lining. It doesn’t stop there. SHMT1 is a co-conversion of the L-serine and tetrahydrofolate, to glycine and the 5MTHF actual end results. So this is an intermediate, kind of little clinical pearl. The GG genotype that you’ve got here, when considered with the context of the MTHFR, is associated with optimal folate metabolism. This is looking at concomitant disease risks reduction associated with dysfunctional folate metabolism. Many who have a poor variant also have issues with the cellular processes, including this gut cell turnover and repair. But in your case, it’s associated with optimal bioavailability and efficient homocysteine to methionine conversion. So here’s the bottom line for you. It’s not the case with everybody, but you’re fine with methylfolate. If somebody didn’t have this genetic sequence, then they may want to be taking folinic acid where you’re getting down to the end of the conversion. In your case you’re fine with folate, methylfolate, more 5MTHF or quadrafolate. Really you’re fine with any of those types that are out there with the MTHF assignment. And then we’ve got MTR: you’re an AA. MTR catalyzes homocysteine to methionine and uses B12 to do it, as the methyl donor in this particular reaction. So this is associated with optimal enzyme activity and conversion of homocysteine to methionine. That’s the AA assignment. It turns out because of this, and I’ll explain some other variants in a second, that you’re fine with methylcobalamin, or the methylated form of B12. If you had any of these other variants down here, we might be wanting to give you a adenosylcobalamin so we’re not hyper methylating you. In studies done on autistic children who found that they had the 5MTHFR. They call it the SNP. Everyone’s got that SNP. It matters what variation of that SNP you have. Right when they found out they had this poor variation of this particular SNP, which is the TT variation, they were giving them in many cases methyltetrahydrofolate, in the methylated form. And in about 15 to 20% of them they were doing worse. And the question was why? And this was one of the answers that Dr. Mohammed was able to answer because they weren’t assigned these other variants that actually helped them to pass that baton in this race and effectively do so in a way that they were able to methylate properly. And then lastly, your MTRR, this reactivates methionine. You have the version AG associated with a slightly reduced enzyme activity, which won’t affect its precursor here, the MTR. So by the way, MTR and MTRR together influence B12 availability, which of course is crucial for DNA synthesis and maintaining the health of the gut lining. But just having this AG here does not all of a sudden screw you up and cause you to require the adenosylcobalamin. So again, we’re still giving you that form of methyl B12. It’s important because this can contribute to things like B12 anemia.
Lindsey:
Which I had following SIBO and and what turned out to be post infectious IBS and for a time positive for pernicious anemia. My hematologist recommended that I get on methylcobalamin. And I’ve essentially been on it continuously for the last 10 years.
Bryce Wylde:
And it would have worked, but guess what in some other combinations and in other folks with the same looking red blood cell count and differentiation, given that, they may not do as well. They may need adenosylcobalamin.
Lindsey:
Lucky guess for him!
Bryce Wylde:
Right. Then lastly, fucosyltransferase, FUT2 the AG is associated with slightly suboptimal enzyme function and plasma levels. This encodes for an enzyme basically, and this is releveant to you, by the way, found in epithelial tissues in the gastrointestinal mucosa and salivary glands. So this SNP shows a significant association with plasma B12 concentrations. And in your case, as you mentioned, this would be the gene that I would associate with poor enzyme function, and poor plasma and B12 levels. All G-allele carriers, whether you’re AG or GG, are associated with significantly lower plasma B12 levels, so what you said doesn’t surprise me at all.
Lindsey:
We’re on page 11 (p. 56 of the PDF). So those two markers that are in the suboptimal variant of AG basically mean that it’s not unusual that I should have to continue to supplement with B12 and folate, methylfolate.
Bryce Wylde:
Yep. And also by the way, combined with a vegetarian diet, these variants are associated with extremely clinically low, and vegan obviously, B12 level. So really important to get on the . . .
Lindsey:
Yeah, I’m not a vegan . . .
Bryce Wylde:
intramuscular in some instances or sublingual various forms of supplementation. Perfect. Yeah, so by the way, most folks that run this test the DNA, we should remind anyone who doesn’t know this, and I’m sure most of your listeners would definitely know this, DNA is one and done. You run this test once your DNA is going to change. The most incredible thing is that where you can’t alter your DNA, you can manage genetic expression, that’s epigenetic. And that’s what we’re talking about, through in this case, a perfect example, methylation. Manage this, by quelling the fire, I don’t care what you call it, subduing and mitigating inflammation, but you’re managing it in a way, your variations of methylation and how you’re able to carry the baton in this relay race with the right types and formats of B12 and folic acid. It really boils down to that for me anyways. There’s other implications here. But that’s really what it boils down to for me, for gut health.
Lindsey:
Yeah, I have always taken it sublingually since that time, because of the pernicious anemia and the SIBO. Right? Okay, so the third area you suggested we focus on is hormone pathways as it relates to gut health. So how are they related? And what does my DNA say about that?
Bryce Wylde:
Let’s just scroll right back down to the hormonal report to keep it simple. Toward the end, we call it hormones fitness and body type (p. 143 of the PDF). We use the traffic lights just to give a visual description of speed. What I want to emphasize here is that again, I alluded to this earlier, but everyone, whether you’re an XX or an XY individual born into this world with those chromosomal differences, we all have the same pathway, hormonally. It’s the speed at which we produce certain hormones that’s going to make the difference here. Again, this is not going to define whether you’re male or female. Within each of those categories, male XY and female XX, you’re going to have this spectrum of androgenized females through to estrogenized females and those in between. Same with men. There’s androgenized guys and estrogenized guys. The team at the DNA company have gotten pretty close now to looking at somebody and phenotypically being able to give a rough estimate of what their hormones probably exude from a genomic perspective. For example, we’re all wearing our heart on our proverbial sleeve here, I’m an estrogenized guy. I’m probably going to have a full head of hair until my late 80s, as my father and both grandfathers did. So that’s just one phenotype. Obviously, the challenge, in my instance, is retaining muscle mass as one additional phenotype. It’s hard for me, so I have to work extra hard. Then you’ll have the guys in the gym and they take one or two days out of the week, and they do half an hour and they’re ripped, and they’re bald. And guess what, they might have that advantage, but then certain hormones an androgenized guy has might predispose them further to prostate cancer, or a BPH (benign prostatic hyperplasia) for that matter. This relates to the gut because it could affect the speed at which you produce progesterone into testosterone, testosterone into estrogen. We know too much excessive estrogen is very proinflammatory, particularly in the gut, and then how you take estrogen and the genes that help clear or metabolize estrogen into their end metabolites. So these are known well for their predisposition unto estrogen-related cancers, breast, ovarian, and colon. And then step three, how you detoxify those, and we’ve been through some of that, but we can reiterate them. So obviously, there’s the hormonal influence on gut permeability, we’re coming to know that. So variants, and we’ll come back to CYP19A1, which is how quickly you take androgens and make estrogen, which affects estrogen synthesis. And that might directly actually influence gut barrier function. There’s the stress response. That’s not just an executive function thing. That’s a hormone thing, and integral to the body’s stress response, causing us to, depending on our variations and genetics, be susceptible to irritable bowel syndrome. Genes like CYP17A1, that you mentioned at the top, that starts this whole cascade here, involved in synthesizing stress hormones. You know that plays probably plays a role. And there’s gut motility, like hormones and neurotransmitters of course influence the speed at which our guts move, right? And how transit time works. Inflammation, particularly sex hormones implicated with an inflammatory response in the gut. So variants here, the androgen receptors, the AR gene, and the variations there affects androgen receptor function, of course, but influences inflammation, inflammatory pathways in the gut. There’s the microbiome composition, there’s immune function, nutrient metabolism, of course, detoxification, all of these things are going to have a major influence on gut health. So your CYP17A1, how you take progesterone in the steroidal sex hormone pathway and produce testosterone, you see this red light, that’s you, you’re slow. That’s actually great. I mean, we call it great, because it depends on everything else I see here. But it’s great because it’s slower, or red light, by the way, does not mean somehow you’re stopped, whether you’re not making enough, it’s not a bad thing, it’s the speed at which you’re taking this. So given that you have a yellow or a green light on the CYP19A1 or in this case, taking testosterone making estrogen. This would be your saving grace if you were green, the speed at which estrogen over spills in the body. But if you were an amber light here, or even a green light here on the CYP17A1 is what I’m pointing at. But then you are an amber or red light on the CYP19A1. That’s a different picture. But I’m painting the scenario of one compensating for the other in terms of overspill, in particular as it relates to gut health of estrogen metabolism. So your variation, and we can flip down to those variations, but I know what they are. So I’ll just refer to them in context of this picture here for you, your CYP17A1, you’re an AA. So this is again, responsible for biotransformation of pregnenolone, progesterone to testosterone, and the Cytochrome P450 cascade. So first step in hormone production critical in determining degree with all your hormones, the rest of their influence on your overall health. So you are a slow converter of progesterone to testosterone, the SRD5A2 is your testosterone into the very virulent dihydrotestosterone or DHT. And the speed at which you do that is average, we’re in the middle in between. Now, one of the things, were talking phenotype, might as well bring it up, it’s not so relevant to gut health, but I can tell you, compared to your peers, your counter, your friends, whoever, that they’re complaining, I mentioned the gym that they’re complaining the degree of what it takes them to work out in the gym and have some level of definition or be lean, and somewhat muscular. And then other friends are always complaining about cellulite and fat retention, all these different things. Obviously, I know, you pay close attention to your diet, I don’t know, maybe there was a time that you didn’t. But even in those times, so long as you did exercise somewhat. And if we consider this, the androgen receptor gene here, and the speed at which you clear testosterone, you don’t have to work as hard as the average person to actually retain muscle mass, and you’re not going to be one of those that really notices cellulite. It’s just the phenotype that you have. I mean, feel free to correct me if I’m wrong, but at least your genes.
Lindsey:
No, not wrong.
Bryce Wylde:
Yeah. So SRD5A2, this is the 5-alpha reductase that converts testosterone into dihydrotestosterone. For you there’s moderate enzyme activity. And you know, we call this potential for elevated dihydrotestosterone. It’s worthy of mentioning at this point. These are genes and depending on your environment, your lifestyle, so many other factors. The only thing it’s going to tell you any conclusive evidence of what’s happening at this moment in time right now are laboratory biomarkers, right? So endpoints, you can test for DHT, right, you can test for these things. Depending on where you are in your life. These are just the signals or the genes that dictate the average amount over your life and where you sit there. But at any given time, you can test for all these different things to know where you are. By the way, in menopause, and I’m sorry to take another tangent, but it’s so relevant in so many things. How you come into menopause, is entirely predicted by where you started this cascade. If somebody is very quick to make an abundant amount of testosterone, and by the way, guess where all estrogen comes from? Testosterone. In guys and and females, it comes from testosterone. It’s the CPY19A1 gene that makes it, in what speed, but if you’re greenlit here from progesterone into testosterone, and you’re greenlit from testosterone into estrogen, what do we call that? We call that estrogen dominant, particularly if how you convert into DHT is relatively slow. It’s like a cascade or waterfall. Everything is going into estrogen. And then if you have over here your estrogen metabolites, I’m giving a hypothetical situation, this is not you. If you’re producing very little 2-hydroxy but a ton of 4-hydroxy and 16-hydroxy, well, then we know what the risks are from that in these estrogen scenarios. Now your estrogen dominant plus estrotoxic, right? So these are these sort of scenarios. That’s not you, thankfully, in again with with you the if there’s potential for producing high amounts of DHT. And I just described some of the various phenotypes. We’ve got to be concerned or thinking about things like PCOS when there’s an elevation or retention of DHT. But your CPY19A1 gene is not at all sluggish or too slow. It’s right right there in the middle, which is exactly what you want. So again, just to remind everyone listening, this catalyzes aromatase and this is the very rate limiting step in the conversion of androgens into estrogens both men and women. And of course, you’re this moderate expression with enzyme activity with modestly reduced estrogen and estrogen to androgen ratios. And again, in postmenopausal, here’s my prediction for you ready? I don’t have a crystal ball, but you’re going to have a quite an easy menopause. You know, I can tell you the reality is that the hot flashes are insufferable, and I’ve had to go on hormones. Oh, you have? Okay, that’s interesting. So the hot flashes may be related to some of those other genes as they pertain to the 9P21 and detox, but, but I would have predicted a relatively easy menopause.
Lindsey:
No other symptoms besides the hot flashes.
Bryce Wylde:
Okay, good. Well, that’s another predictor. By the way, these are all symptoms that the body uses to prepare, inevitably, this shift. So the speed at which you actually go through menopause is another thing, and nothing I can predict through what I’m seeing here. But how quickly obviously, your estrogen supplies dwindle, controlled by other genes, would be would be related in this as well.
Lindsey:
So first question. Is there anything in here that predicts that I’m going to be low on progesterone?
Bryce Wylde:
So we don’t look at the genes that ultimately cascade down from cholesterol, because they’re not as important. Obviously, if you’re on a statin, and certain things suppress cholesterol, or some of the other precursory . . . pregnenolone, and so forth. But what this suggests is the amount of progesterone that is otherwise circulating at any given time, is otherwise average to higher than the average individual. So and that doesn’t mean menopause because those are all going to blink a little bit. But here’s really what I want to drive home depending on what kinds of hormones people are otherwise supplementing, bioidentical hormone replacement therapy, there are certain qualifications we like to look at. And this is relevant to gut health, very relevant to gut health. If you are estrogen dominant, and estrogen toxic by taking progesterone even on its own, what’s it going to do? It’s turning into testosterone into estrogen. It’s not exclusive, you are producing more of that stuff. So if I’m looking at you, and I’m looking to determine a candidacy, if you will, for BioIdentical Hormone Replacement Therapy, or even regular HRT, you’re a great candidate. Anyone looking at this would say, or any of our team anyways, would say yes, she’s actually qualified with the exception. And it’s a mild exception down here. This is what we’re going get into step two here is looking at the degree of metabolite production again, the speed at which you produce these metabolites. In an ideal world, you’d have a green light over here, in an ideal world, and what this is a 2-hydroxy estrogen I’m looking at controlled by the CYP1A1 variant. And the reason I say that in an ideal world is because being slow on the protective 2-hydroxy is to suggest you’re a little more at risk studies show. And then over here, the 4-hydroxy, in an ideal world, it’s fine that it’s this yellow variant that, you know, it would be red and 16 would also be red. So how we work this through though is, and you’re very familiar I’m sure with the research around indole-3-carbinol or diindolylmethane (DIM) and some of these cruciferous family of vegetable extracts, that this helps flip the switch on this helps to slow down the 4OHe and over to the 2-hydroxy estrogen so helps to increase or helps to speed up the metabolism of the estrogen and clear it.
Lindsey:
So eat my broccoli?
Bryce Wylde:
Eat your broccoli. Bowls and bowls of it. So in the gut health circles, depending on your FODMAP assignment or how well you do on some of the insoluble fiber levels and so forth. And obviously that’s a whole different story. But yes, at the very least take an extract and I tend to prefer a diindolylmethane over indole-3-carbinol. I think in these instances, anyways, I don’t think you can eat yourself to a therapeutic range of broccoli.
Lindsey:
I have at various points taken that for various and sundry reasons. So definitely something I can go back on.
Bryce Wylde:
Yeah, I think so. I think it’s indicated for you. So far, I think there’s two things that I would really consider in your daily regime. And that would be the tocotrienols and some indole-3-carbinol, or probably even better, some diindolylmethane (DIM). And then this step here that we’ve already somewhat discussed today at length, glutathionization. We haven’t talked about the detoxification ramifications of catechol-o-methyltransferase, which is also involved in executive function, very important in methylation and converting all the neurotransmitters into active metabolites, etc. But it’s very important here in excreting estrogens. Now, the reason, and I’m just going to highlight this real quick, you’re seeing a red light on GSTs, and our algorithm works in very mysterious ways. Sometimes this is one of them. If your GSTP1, which is true, you have the AG variant, it’s going to show up automatically, even though you have a great GSTT1, two copies and a great GSTM1, two copies, your SOD, you know, hybrid variant AG, and your GSTP1. So that’s why it says considered suboptimal. So the other thing is maybe, again, when we’re talking gut health, I still think one of the best things to consider for folks is upregulating glutathione. And I think, if you do a quick PubMed search, there’s like 32, or four, something like in the realm of low 30 studies have been done on supplemental glutathione. And 30 or more of them have basically resulted in either no effect or very little effect. And I think what the studies show in summary is that yes, the glutathione that you might consume in glutathione format, whether it’s liposomalized or otherwise, reduced, acetyl- or whatever, is probably entering to the system, but it’s not getting into the cell, intracellular, whether it’s the cells of your intestine or into your red blood cells beyond homeostasis. So it’s probably doing some antioxidant good outside of that, but it’s not getting beyond homeostasis into the cell. So we like to recommend precursors.
Lindsey:
Like NAC or glycine?
Bryce Wylde:
You got it. NAC, glycine, exactly. Alpha Lipoic Acid, selenium, a little bit of selenium, or three Brazil nuts a day, non irradiated, organic, if possible, Brazil nuts. But there’s also some interesting ingredients, I think out there worthy of further due diligence by anyone listening to this, and that’s gamma-glutamylcysteine. So some interesting studies out of Australia, taking this gamma-glutamylcysteine, seems to actually upregulate glutathione intracellularly. Beyond homeostasis. So it’s like the direct precursor. Anyways, all of that to say, we’re huge fans of precursors to glutathione. We don’t think glutathione itself is really going to work, it’s probably just going to dissolve in the stomach and in the gut, and not really do. . .
Lindsey:
What about S-acetyl-glutathione?
Bryce Wylde:
Any of those variants, you look at any of those things, and it just doesn’t survive, it just gets taken down.
Lindsey:
Well, it’s a lot more expensive, so certainly easier to get the precursors.
Bryce Wylde:
And there you go, exactly. So in a generalized summary of detoxification and gut health, and methylation and gut health, we’re talking about elimination of toxins, liver-gut axis, microbiome interaction, cellular repair, that’s so huge, immune regulation, all these things factor in neurotransmitter synthesis. We didn’t get into that. But obviously, we look at the whole brain-gut axis and executive function, energy metabolism and methylation. All that plays a role and the interaction between detoxification and methylation oxy toxin elimination, microbiome, I think I mentioned that, hormone balance, we just finished some of that. Both detoxification and methylation influence hormone metabolism and elimination, which can impact various aspects of gut health as well, including motility that we very briefly alluded to, and even immune function. So you’re getting to see how all of these things, you can’t look at any single gene on its own. All of them play a significant interaction, and they need to be looked at in context of pathways. And we’re very proud of that at the DNA company, not just what we look at and how we report on them. But the science that supports these various pathways and pathway interactions, I guess, would be the quick and dirty summary.
Lindsey:
Do you have time for one more question?
Bryce Wylde:
Love it.
Lindsey:
Okay, so this is a little off topic. But one of the reasons I was really excited to have this report done by the DNA company was because in my 23andme results, when I ran them through Genetic Genie, it indicated that I had APOE 4 and 4, which is the worst genotype for the risk of Alzheimer’s. And I recall reading that that meant I had something like an 85% risk of having Alzheimer’s by age 80, but correct me if I’m wrong. So I was waiting for independent confirmation of this. And so I was really relieved when you ran this report, and I saw that I only have APOE 4 and one APOE 3. So can you tell me a bit about this and the degree of difference in risk profiles for 3 versus 4 and what people can do who have the APOE 4 genes and other genes that are relevant to Alzheimer’s?
Bryce Wylde:
Absolutely, yeah. So starting at the top with when we’re thinking about where we’re getting our information from, or that is to say the results of a genetic report, we have to consider where it’s coming from. And ultimately, unfortunately, some of these genetic reporting companies that are involved in looking at a tremendous amount of genes all at once, this is really more of a cost savings iInitiative, or let’s call it a business model. They can’t run small runs of gene sequences. And this gets a little bit complicated, but just save it to say they’re running tens of thousands, so your entire genome essentially, at one time. That’s going to lead to a varying degree of inaccurate reporting. And it’s quite widely available, the literature boils this down, it’s basically 15 to 20% of false positive on the APOE4, so either receiving a 4 or a 3/4 or 4/4 a variation wrong 15-20% of the time. I probably shouldn’t say this, I’ll just use a very famous TV doctor had this done. And we did these genetic tests for that person, very unique, actually, presentation. But I’m saying this because he reported his variations on the air. So but I’m just holding back a little on the story. But at the end of the day, same kinds of situation went down as I’m assuming went down with you is he was falsely reported on. We correctly reported on, and here’s why we’re able to correctly report on these. It’s because we run very small runs, really small batches of genetics at a time, so the chances of making a mistake is very low. When you look at the literature, what you have to understand about these studies, by the way, see, I’m showing you this on p. 4 of the cardiovascular report (p. 45 of the PDF). That’s because we don’t report APOE in context of some kind of dementia report. So we’re not making anything that we can talk about it in context of cognitive decline. Dementia is very relevant to that. But we report first and foremost on this cholesterol carrying capable capability of the apolipoprotein. And that plays a role. But so you look at these populations, and you see, those that have essentially had diagnoses of Alzheimer’s, that were extrapolated, and then looked at, depending on literature, you read, 30 to 40% of those with Alzheimer’s had an assignment of genomic APOE 3/4 and upwards of 70% had 4/4 variants. But you can’t just jump the gun and so quickly reverse engineer that to mean, if I have an APOE 3/4, I have a 30 to 40% increased chance of getting Alzheimer’s. And really, there’s so many different factors involved, as we all know, right? Diet, lifestyle, sleep, can get into so much here. But so there’s a definite association. We don’t report on this as the Alzheimer’s gene. We could talk Alzheimer’s, because having your variation here of a 3/4, there’s implications of again, cardiovascular disease, coronary artery disease, ischemic stroke, and we haven’t talked about the combination. But putting this in combination with the 9P21. It’s definitely a highlight risk for me for you. And it’s something that you want to take away from this report outside of gut health and its implications, is cardiovascular disease. So this is very much an old story of cholesterol being part of it, obviously size, particle size, oxidative cholesterol, how angry it might be and how quickly it might want to deposit within the lumen of the artery lining. But when we combine APOE, as a 3/4 with a 9P21 multiple G, we’re much more concerned about the predisposition of inflammation that warrants the deposition of that cholesterol, right? Does that make sense? So yes, you know that the studies are there. By the way, third ingredient for you, for me, anyway, would be a very bioavailable form of curcumin. And there’s multiple ones out there. I like the liposomal curcumin in this case. It’s all about bioavailability because it doesn’t easily, speaking about the gut, doesn’t easily get through the gut, into the general circulation. So piperine or pepper can help that. But liposomal or micellized. Micellizing is getting it to even smaller, tiny little lipid particle size that can get absorbed easier. So yeah, I’d say with this gene, we like to make these recommendations in combination with other factors, consider that curcumin is advisable for you. But that’s a long way of saying there’s some inaccuracies in certain other companies reporting on this gene. We can’t take it out of context and say it’s a direct upregulation or assignment to getting Alzheimer’s. But at the same time, can you mitigate or do certain things given the rest of the genome pathways that you’re expressing risk. And I think yeah, you can, that’s our whole MO is what can we do through diet, lifestyle and supplementation to tweak or mitigate genetic pathway expression?
Lindsey:
Awesome. Well, this was all super interesting. And I love hearing this about my genes. I wish I could go through the entire report with you, but I will certainly read it more in detail myself. I really appreciate you giving your time to this. And we will include links on how to order your own DNA report from The DNA Company in the show notes.
Bryce Wylde:
I appreciate you having me on.
Lindsey:
Yeah, thank you so much for being here. Any final thoughts?
Bryce Wylde:
I just think understanding our genetics and our gene pathways is an incredibly useful starting point to knowing what more we need to focus on. A lot of people are confused about, if they’re biohacking, or what might be the underlying – we hear this term all the time underlying cause – so you know, obviously genes and environment play a role and how we grew up and all these different things. But I think it’s a great starting point for most people. And if you think about it, it’s a one and done test, which I also love, so you’re spending in, but you never have to do the test again. And it informs on so much more of what you want to put your efforts toward and I think that’s what people are so confused as to where do I start. Well you know, what’s a great place to start the journey, start the process of wellness biohacking. Understanding potentially what other physicians, clinicians, consultants, like yourself, you might want to consider talking to to help you navigate and wade through. There’s so much to know and learn, right, but it’s a great starting point. This is your instruction manual. And if you don’t know it, you’re at a disadvantage.
Lindsey:
Yeah. And I think for people in particular who have very complex health problems that are deep like chronic fatigue or fibromyalgia or some combo of gut issues and mental health issues and something else, that’s the kind of situation where I think that something like this would be useful.
Bryce Wylde:
Can we have time for just a quick anecdote?
Lindsey:
Sure,
Bryce Wylde:
Okay, thank you. So on that note, this is where we see incredible stuff come out of the weeds. So in our clinic and I mentioned this is going back top to the top talking with Dr. Mohammed, I give him such kudos for figuring this out. The light bulb that went off. We had all these young female patients at P3 Health coming in, and you know, what you call out for, what you see more of and do well for, you get more patients, right? So we had all these women come in with chronic fatigue and fibromyalgia and misdiagnosed Lyme and we did well at diagnosing Lyme, still do and couldn’t figure out. It was a huge pool. There was like dozens of these women and again, in their mid to late 20s. Otherwise should be healthy, eating healthy tried everything. Okay. What did they all have in common genomically? I’ll just cut to the chase. They were null variant detoxifiers; they did not have the instructions to properly detoxify. In combination. The two most striking things, there was a third, but it came third, distant third. The second thing, estrogen dominance with estrogen toxicity. So alluded to that a little bit. Third thing, distant third, methylation, poor methylators, but nonetheless poor like terrible detoxification, methyl estrogen dominant, estrogen toxic. This is a story more about what we got them off versus what we gave them. What did we take them off? Birth control pills. They were probably just adding fuel to the fire so they had these predispositions, but they were taking birth control pills, hyper dominant estrogen, not able to clear it. Because that COMT and GSTs are reliant on that information, they’re genetically there to get estrogen out of the body. So just dumping more estrogen, like fuel right onto the fire. So yeah, nine times out of 10, maybe more, taking them off their birth control pill, has solved their chronic fatigue and fibromyalgia.
Lindsey:
Wow. Very interesting. Well thank you so much for your time. This was awesome.
Bryce Wylde:
Thanks, Lindsey. I appreciate it. Thanks for all you do.
Ifyou’re struggling with bloating, constipation, diarrhea, soft stool, acid reflux, IBS, IBD or any type of chronic disease, etc. and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me (Lindsey). We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
Adapted from episode 109 of The Perfect Stool podcast and edited for readability, with Lindsey Parsons, EdD, Gut Health Coach and Jordan Power, an ulcerative colitis sufferer who reversed his disease after doctors suggested he have a foot of his colon removed.
Lindsey:
Like many people who’ve turned to alternative medicine, you were able to reverse your ulcerative colitis. And you may have had an exceptionally bad case, because as I understand it, your doctors were recommending that you remove a foot of your colon. So why don’t you tell us the story, from the beginning, about how you ended up with ulcerative colitis, and then what you did to reverse it?
Jordan Powers:
Sure. My background is that I come from a family of two doctors. My parents were doctors, and my sister’s actually an ER nurse. I come from the very common medical establishment pieties, let’s say. When I was about 18 years old, I went on multiple rounds of Accutane. It probably started when I was actually 17. When I had that third round of Accutane, in the middle of it, I got extremely sick to the point where I was admitted to hospital. I had dropped about 25 pounds in a period of about two and a half months, and I looked very sick. My bloodwork was terrible. No one really knew what was going on. My mom sent me for some testing, and eventually they diagnosed me with ulcerative colitis. The connection to Accutane hadn’t been made, and the people in the US hadn’t sued yet for multi seven figure judgments. They made that connection probably 10 years after I was diagnosed, and I signed up for the class action then. I don’t know for sure if that’s the connection, but I don’t have a history of any inflammatory bowel disease in my family. Colitis just came out of nowhere.
Lindsey:
Let me pause you for a second. So Accutane, just to clarify, is a drug for acne, and I know it’s high in vitamin A. It’s not just vitamin A, though, is it?
Jordan Powers:
Vitamin A acid, I believe. All I remember really is that it mentally drove me into a total depression. Then all your orifices and your mucous membranes dry up, because the idea is that the medicine dries up your sebaceous glands. It does work for acne. Don’t get me wrong, it absolutely works.
Lindsey:
Yeah, with the small side effect of ulcerative colitis, right.
Jordan Powers:
Then you have a disease for life.
Lindsey:
I’ve heard of other people having vitamin A overdose from it.
Jordan Powers:
They pulled it off the shelves for a period of time. I don’t know if it’s still off. In my book, I talk about a place called Kitava, in New Guinea. It’s a small island where they don’t have the chronic diseases we have in North America. Their teenagers don’t have acne. They don’t go through that requisite period where you have to get acne.
Lindsey:
I think anyone who doesn’t eat a bunch of processed food and sugar also has the potential of not having acne.
Jordan Powers:
Yes, it’s true. But you know, it’s just we think it’s just part of life. You’re a teenager with acne. That’s just what happens.
Lindsey:
Yeah, not at all. I told my kid as soon as he got his first real zit, that if he goes off sugar, he wouldn’t have acne. The fact that his entire diet consisted of processed white carbs made it hard. Not that I was the person who purchased those foods, just a disclaimer, but even so, that was his diet. The sugar alone wasn’t enough, but he actually did it. I couldn’t believe a child had that level of willpower to go off sugar like that. He’s pretty much stayed off it other than brief pauses for holidays like Thanksgiving and Christmas.
Jordan Powers:
Wow, did you get them off seed oils, too?
Lindsey:
We didn’t really use them in our home. So other than in the processed foods that I wasn’t purchasing, yes, he was mostly off seed oils.
Jordan Powers:
Right. Okay. It’s just that they’re in 99% of restaurants, if you eat out.
Lindsey:
Right. So if he ate out, of course he couldn’t avoid them.
Jordan Powers:
Going back to my initial diagnosis, it was the age old tale of the doctor sitting you down and saying these are the only options. These three drugs are the only options available, these three drugs and steroids. There’s no cure, and no discussion of holistic treatments. At the time, I was still in that complex, right? I’m not really blaming my parents here, but I grew up with a certain conditioning. And the people that question that conditioning are often cast from polite society and deemed the crazy ones. Then I grew up and realized it’s actually the inverse. And the reason that they were cast from polite society is that they’re a threat to some sort of neoliberal order.
That was a real period where I just went on tons of medication, around eight pills a day, steroids, and hospital admissions. I saw my health get progressively worse. Around the time of my mid twenties, it stabilized. I do want to note also that I was eating well, I wasn’t eating a lot of bad food, but when you have that delicate of a microbiome, anything can really set you off. Then there was a period about a year and a half ago, where I went to South America and the combination of seed oils and alcohol and processed food and all the other things I was having set off what I called the train. With Colitis and Crohn’s disease, or inflammatory bowel disease, once you start going, it’s really hard to stop the train. So I’ve had multiple vacations ruined, my trip to Israel, and my trip to Colombia were both just completely ruined. I came back home and I couldn’t get it under control with medication or with steroids. I just couldn’t stop it.
And so I sat down with my doctor after two colonoscopies, and he said to me, we can basically just cut out a foot of your colon, and then that’ll solve the problem. I’m not really a spiritual person, but there was really this moment where I was sitting in the room, and I said to myself, “Yeah, I don’t think this is in the cards for me. I don’t think this is part of my life.” I don’t know if that’s a level of denial. It could be. I just thought, I don’t need this. I came home and went on the internet and I started searching on YouTube. I stumbled across all kinds of people and started going on alternative paths. I call this experience opening boxes of horror. I was looking into what’s in our beauty products, what’s in our cleaning products, what’s allowed in North America that’s banned in Europe, all these different boxes that I kept opening.
I had a really protracted discussion with a man who worked in cosmetics consulting for some major companies. He would tell me these horror stories where he would tell them that this product is going to cause lung cancer, and they would just say, “Thank you for your service, goodbye.” I learned that there wasn’t a lot of money in integrity. I got so freaked out between my YouTube rabbit holes and discussions with him, that I just went on a binge, and I got rid of every chemical in my house, starting with cleaning products and beauty products. Then I found alternatives, and started really adapting an elimination diet through Paul Saladino, the carnivore MD, on YouTube. Within 30 days, it was gone. When I say gone, I mean really gone. It was the best health I’d had in my entire life after just 30 days.
Lindsey:
Wow. Can you summarize the diet that you went on? And then I assume you reintroduced things after, so can you tell me about the progression? Did you go full carnivore?
Jordan Powers:
No, so what I did was sort of carnivore: fruits, honey, raw dairy, and a bit of potatoes. Potatoes has just been something that always made me feel good. I don’t know if it’s the prebiotics. Before that I had never experimented with raw dairy. I heard the tales that it was going to kill me, but then I start doing research for my book. It said there’s only a one in 6 million chance of dying, and that there’s a much higher chance with cantaloupe and spinach and all these foods. So I got my hands on some raw dairy, because where I live, it’s illegal although there’s ways to get around it, which we don’t have to get into, but people can figure it out on their own. Raw dairy felt great. When I drank it, I felt like it was connecting with my body, whereas when I had pasteurized dairy, I would feel this inflammation in my body. So it was really just the meat, the raw honey, the raw dairy, fruit, and the potatoes and I stuck with that for about 30 days.
Obviously, it’s boring, but you know, when you’re that sick, you’ll do anything. Then the combination of swapping in different products in my house, starting with switching shampoo for a shampoo bar, skin products for beef tallow moisturizer, getting off the chemical sunscreens, and then really just cleaning my house with just rubbing alcohol and a little bit of soap and some essential oils, or some baking soda and vinegar.
The craziest part of this whole thing that also happened to me is that before I just assumed that I was depressed and anxious. I thought that was just my destiny. I’m 50% Irish, and it’s just how we are. The added bonus of this whole thing is that I would wake up after battling these illnesses off and on for most of my life, treating them with multiple SSRIs, and now I don’t think I have these mental issues either. I don’t think I actually am depressed or anxious. I don’t feel depressed, I can manage stress situations now in a different way and the modulation of my moods. That was the craziest part, more even than the colitis recovery, was to see the mental aspect. The way that you approach the world on a daily basis is affected by this. Even when my dog died during all this, I handled it in a way that I don’t think I would have if I didn’t have a stable mind. I was at peace with what was happening and I wasn’t trying to fight it. I wake up now and I say that I’m a different person. I don’t even recognize the body that I live in now.
Lindsey:
That’s amazing. Getting back to sort of the diet changes, what were the most dramatic things that you removed from your diet for this 30 days that were really transformational?
Jordan Powers:
This might be controversial, but spinach and kale were terrible, with the oxalates. Kale has great PR, so you read everywhere, you got to have kale. I would eat kale, and I would feel terrible. I would have the runs. Broccoli was terrible, any cruciferous vegetable was terrible. What I would do is I would make an anti-shopping list. I’d have my shopping list on the one side of things that I knew were fine. Then every time something would bother me, I would just write it down. I had to be hyper attuned to my body at that point. Most people are just like bots. We go through life, and we’re just eating things, and then 12 hours later, we don’t connect the dots with the food. So I created an anti shopping list, and I would just write down spinach, kale, broccoli, any white breads were a no. Obviously, any processed sugars were a no. Any meats where the animal was eating seed oils, hormones, or antibiotics I had to get rid of.
Lindsey:
So you went to high quality pasture-raised meats, and that kind of thing?
Jordan Powers:
Absolutely. That was another one. I realized that I can eat a steak and not feel bloated. Before I thought I hated steak, because I’d feel sick, and that was that. With the fruits, I would go organic as much as possible, and I would wash them in apple cider vinegar, or I would do different things to make them as clean as possible. I also started chewing my food slowly. That was an interesting thing. Before, I was always rushing, working, trying to get things in my body, but proper nutrient absorption happens through chewing the food. Even with my mineral water that I drink, I now swish it in my mouth and kind of let it absorb into the gums a little bit before I swallow. That’s a little trick that I do.
Lindsey:
That also warms it up.
Jordan Powers:
Yes, and then supplementation-wise, I went on to beef colostrum, because it’s really been shown to regenerate the intestinal lining. That was a big one for me. The biggest thing was also that I got rid of all the crap supplements I had been taking. Instead I just went down to beef heart and beef liver every day as a supplement, because I don’t love the taste. So that was the combination. And then I would try different supplements, zinc and stuff like that, but I really came down to the belief that high quality food cannot compare to the supplements that are shipped to your house with God knows whatever plastic and whatever fillers are in them. I just don’t think they’re comparable unless you find a really good supplier, so I really only take about four or five supplements now.
Lindsey:
To clarify, it doesn’t sound like you cut out all of your fiber when you did this 30 day diet, which is a more traditional colitis flaring diet.
Jordan Powers:
No, you know, the interesting thing about colitis is you oscillate between constipation and diarrhea sometimes, just because your body is off. So I did get the fiber from the fruit and select vegetables that I was eating, like carrots, that weren’t bothering me. But for the most part, the only vegetables I do eat now are carrots, some onions, some tomatoes. That’s all that I consume in the vegetable world because even when I used to have vegetable soup, I would feel disgusting afterwards, which seems like it runs contrary to so much of what we’re taught when we’re younger.
Lindsey:
So you’ve sort of stuck with this more limited diet.
Jordan Powers:
Yes, and I feel great. People tell me that my life is so boring, because my grocery list is about 15 items. But I don’t care because people don’t understand what it’s like to have your life consumed by a disease. There’s nothing that a variety of foods is going to make up for. I don’t want to go back to that horror and that darkness that I lived in, and of course, I do cheat. I’ll go on vacation and I’ll have dinner here and there. But I am fully functional now, it is unbelievable. I went for a scan with my doctor. Again, medical professionals can be pompous, and I say that as someone who’s parents are doctors. The doctor was looking at my colitis scan and he really just asked me what was going on because there was no evidence of disease. And I told him what I did, and he said that the good results were probably just a medication that I had switched to.
It’s so interesting to me, because I feel like they think that holistic medicine can’t work in marriage with modern medicine. It can’t augment it or kind of replace it. They feel like it’s a threat to their ego and who they are and what they’re taught. And I will say that I really give credit to my mom, who’s a GP, because she has really opened her mind up to the holistic world. She has told me that if she did her whole career again, she would really focus much more on the holistic route. Because, like I said, we call it the Pandora’s box of horrors. We open up something that we’ve been taught over and over, and it’s just horror after horror unveiling itself.
Lindsey:
Yeah, I look at my doctor and sometimes I think she’s just leading a life of quiet desperation. As a doctor, you’ve got this brief amount of time to talk to somebody and you don’t really know or understand all the stuff they’re taking, because for example, I’ve got a pile of supplements that I’m on and, and she doesn’t necessarily know how to solve my problem. I’ll just ask her to run the tests I want, and I’ll take care of the rest. God bless her. She does that.
Jordan Powers:
It’s also their time constraint, they have a period of 10 to 15 minutes to see you, and there’s no way they’re going to ask you about your diet and analyze your microbiome.
Lindsey:
Right. No, of course, they’re going to look at your medical record, and they’re not going to remember you because they see 20-30 patients a day, and they’re going to look and only quickly take a summary. And then that’s it. They’re not going to remember all of your history and everything else unless you really stood out to them.
Jordan Powers:
It’s funny, because now I’m in this holistic mindset. And I went to a doctor with these white spots on my skin called idiopathic guttate hypomelanosis, and it is just little white spots on your skin. The common belief when you google this is that it’s just sun damage. You get too much sun and you have these white spots. I’m sure that true for some people but mine kind of just showed up very quickly, within a three to four week period, I had them all over my legs and arms. And I went to this doctor who was like the biggest dermatologist in Toronto, double board certified, a hotshot, and he said it’s sun damage and to just put sunscreen on and stay out of the sun. I told him that I thought something else is going on here. It just appeared out of nowhere. And I had just been in Thailand, which was a hint.
So I then I went to a holistic doctor that I pay. It was the same diagnosis; it’s a fungus on your skin. This is how you treat it. He said do this and this, take these supplements, put this antifungal cream on and within three weeks, it’s gone. At the end of the day, they both diagnosed it correctly. But you had the first doctor saying there’s no options available for you. And then the second doctor is saying there’s something going on here at its core. That’s very much like the colitis thing. Why is my body attacking itself? What purpose would that serve? And why are these illnesses not in these places like New Guinea? And to start with those questions sets you off on a different kind of path.
Lindsey:
Yeah. So you never went on a biologic, did you? Was that offered to you? Or did you not get to that point?
Jordan Powers:
It was offered to me, it was around the same time at the surgery. And I didn’t do it because it was about $1,000.
Lindsey:
Unfortunately, the side effect for people that go on them is suppressing your immune system. One of the biggest dangers, of course, is getting cancer. So of course, there’s a trade off, my ulcerative colitis might go away for a while, but I may get cancer in the meantime.
Jordan Powers:
Yeah, I feel like you maybe have the same belief as me, that the body, if you just leave it alone, it’ll just fix itself. But once you start one thing, it’s a domino effect where you throw off the whole homeostasis of the system and then other things start popping up. You know, I’m on an SSRI for this and now my sex drive is down. So I need to take this other pill and then it’s causing this and suddenly you’ve got five side effects going on. Where you should instead just conquer the question of why are you depressed and what is the impetus for that depression? But they don’t have time.
Lindsey:
Of course, right now it seems like with the mental health medications, especially if you get beyond just depression and anxiety and into like bipolar, that kind of thing, you can start piling one medication on to another and all of a sudden there’s teenagers who have five mental health medications and often the parents at some point go okay, something’s not right here. We need to make some lifestyle changes. Usually you have to go relatively far down that route before you start realizing that it is insanity. My child should not be on five medications.
Jordan Powers:
It’s also the same thing with the skin. People tell me that my skin’s never looked better and ask me what do I put on it? And I’m like, beef tallow with raw honey mixed into it. I just bought it off the internet. That’s all I do. I don’t even wash my face. I just put that on now. I used to put on a cleanser with alcohol in it that would strip the oils and then I would put on a toner with 48 ingredients. Then I’d put on some other cream that was in plastic and a truck. I would do all this and my skin looked worse. I had more breakouts, I just put this $35 beef tallow with raw honey on every day. And that’s literally all I do, and my skin looks better than most people. It just goes back to the idea of just leave it alone. Leave your skin alone. Just leave it alone, because by complicating things you’re creating all these different problems for yourself.
Lindsey:
Years ago when I was in college dated a guy who asked me why I washed my face with anything, because he just washed his face with water. I decided to try that. And ever since I’ve washed my face with nothing but water. I have never had skin issues of any sort.
Jordan Powers:
I think you just mess up the system.
Lindsey:
Yeah. It’s just a big industry trying to sell us more stuff. So it sounds like you really believe that removing toxins from your house, and your diet was a big part of the puzzle, what makes you so sure that that was a big reason for your healing?
Jordan Powers:
Well, when I wrote my book, I linked to a bunch of studies, which all showed that when you mess with the microbiome, that’s when you start having problems. 50% of the diversity of our microbiomes has been destroyed over the past few decades. So I think when you mess with anything, that’s a problem. For example, if you’re eating a plate of something, and there’s still detergent on it, then you’re mixing that with your food. What is that doing to your gut? Even drinking tap water, the fluorides and everything that’s in that is terrible. It really was these conversations I had with this guy.
And then when I wrote in my book, don’t use this product, don’t use this product, it’s been linked with lead or heavy metals. I link in my book the various studies out there for these different things. So I’m not this guy saying I’m just anecdotally making this up, right. I can tell you, not just from the conversations with this consultant, who’s 30 years in the cosmetics business, and the stuff I’ve watched, but also the studies I put in my book. Just anecdotally, from myself, when I introduced those things into my life, because I am hyperattuned to my moods, I can tell you that they messed me up. I noticed that when I go on vacation, because then I can’t filter my tap or my shower water. When I’m on vacation the combination of having to eat seed oils and having to have certain chemicals and stuff like that in my body, I start to notice that I snap more at people. I realized that eliminating certain foods and chemicals meant that I wasn’t triggered by things. And I wasn’t snapping at people. There’s moments on vacation where I’m just a little more snappy than usual.
Lindsey:
Yeah, and you should, in theory be more relaxed on vacation.
Jordan Powers:
Absolutely. I think I snap because on vacation I’m just introducing bad things to my body. I really do believe that it’s been almost a year now where I’ve been off medication, I am in the best health I’ve ever been in my life, mentally and physically. But I don’t get too confident, because I do believe I’m still teetering, and I will be teetering for another year or so. I’ve talked to, there’s a guy named The Holistic Nick or Kenny Honnas, also guys who have cured their colitis. They say it takes a couple of years to really get yourself back to a point. So I try not to risk it, and stay as diligent with things because I don’t want to backslide. There are moments where I feel a backslide, when I’ll go for dinner with some friends or have a little booze or not get great sleep. I can see myself going there.
But it is very, very scary what is in a lot of those products. Even stem cell creams are barely tested, and they put those on the market and people were just slathering them all over their face, and they mess with cell replication. No one knows the long term effects of those. A lot of these clinical trials when you look into these beauty trials for different creams, it really comes down to we gave the cream to 60 women for 90 days and none of them got a rash. Go buy it at the CVS. People think there are a lot more guardrails in place to protect them. There’s also things in your food and beauty products that are banned in Europe but allowed in North America.
Lindsey:
Yeah, like food dyes, for example. I spent many years fighting to get the food dyes out of the food in the Montgomery County Public Schools outside of DC in Maryland. We got rid of almost everything. I would say the only thing that remains are natural caramel colors that they put in meats, because it’s almost impossible to get those removed, given the quality of meat that they get in the school system. We got them out, we did a lot of good things.
Jordan Powers:
Wow, good for you. It’s the little battles that leave a mark on the world. You made a change for people. Some of those changes might not even be so tangible for people, but they might even go, “Well, I feel better this week.”
Lindsey:
With food dyes, it’s not that everybody’s affected by them. But there’s a certain subset of kids that have ADHD kind of symptoms because of food dyes. My partner who started the nonprofit with me, called at the time, Real Food for Kids – Montgomery, she had a daughter who was one of those kids that reacted to food dyes, and she did crazy stuff when she was on the food dyes.
Jordan Powers:
I’m newer, and I’m not trying to be a health expert. I just really wrote this book because of my experience. A lot of people asked me about my healing process, so I just wanted to get this out there. You seem like you’ve been immersed in this for a longer period of time. Do you feel like you’re used to the way that people will dismiss you, or sort of pretend that you’re the crazy one because you don’t want toxins in your life?
Lindsey:
If it’s a doctor, I don’t open the door to even let them say anything about what I’m doing. I mean, I know my GP is good. But I’ve definitely had one bad experience with a gastroenterologist completely dismissing and belittling me. After that, I decided I’m not even going to share anything. I’m just going to come here, tell them what I want or need, take whatever piece of advice that’s within their conventional medical paradigm, and then just do the rest on my own.
When it comes to other people outside that, I do find that there are certain people who don’t understand my work. This maybe comes up the most when you know someone who has cancer, because that’s when you’re feeling this desperation. There’s so much I could tell you about what you should and shouldn’t be doing, and about ideas and people to look at. But you can only reach out so much, because everybody in their life is doing the same thing, right? You’re not the only person giving them advice. Especially if you’re not that close to that person. Usually things get crazy when you get cancer, right? Like all of a sudden everything drops out, but you have to focus on the most important things. So I don’t think they can even receive all that input, because they aren’t even checking email anymore, or because they’re more worried about just living and dying and things like that.
So it’s happened a number of times that you’ve seen somebody get cancer that you know, and love, and you just can’t do anything if that’s not their paradigm. Two of the people I knew who died of cancer at age 50, their parents were doctors. And, of course, they were not as open to alternative things. I mean, somewhat one of them, but the other one was completely closed off to it. And there was nothing I could do. I couldn’t come to their homes and force food down their throat. You know what I mean? I couldn’t change their diets. I couldn’t even get them to consider supplements. I certainly couldn’t get them to consider alternative practitioners. There just was nothing I could do. I mean, I did my best, but it was it was frustrating.
Jordan Powers:
Yeah, it’s a very isolating existence to be heterodox on any subject. Now I’m heterodox on health. I was already heterodox on the media, because I’d worked in IT for 12 years. So I think I needed that conditioning to question the establishment in order to then also be able to take in alternative health information. But a lot of people, I don’t know what the wiring is in their head, but they need experts, and they need to just go with the flow, and they need to follow.
Lindsey:
Right. I mean, you have to feel like you’re doing the right thing for yourself. And I guess you have to decide what that is, and then close your mind to everything else. Because if you keep it open, then there’s all sorts of quack jobs who are trying to push all sorts of things that have no peer-reviewed evidence behind them. There’s a difference because there are actual studies on this, even if this may be a newer idea, there’s still initial studies. By the time it gets into the conventional medical paradigm, it’s 20 years behind. When it becomes part of the standard of care, at that point, you could have been using it for 20 years because it takes that long to get into the standard of care.
Jordan Powers:
One of the things I was talking about with someone who was going to get an MRI my life is that it’s coming out now the dye they use in MRIs is heavily linked to cancer now. People are getting MRIs every day with this stuff. And now they’re trying to ban it in certain places. So there’s the irony of going for cancer screening and to then take a cancer-causing agent at the same time. I find myself trying to not get too paranoid because it’s just not feasible. I’ve kind of stopped opening boxes because every time I open a box, I find more horror. It’s the same with wars and anything else, so I’ve pulled back on that.
I think there’s maturity when you tell people your experience and you’re standing in front of them, and you’ve cured your disease and your depression, anxiety. In that case, they can’t really deny you, they can’t deny looking at you and seeing that you’re functional and you lead by example. And so that’s also why I wanted to write this book for people. I say to people, “Hey, I’m not a mirage. I was the person that you saw in the hospital multiple times who was very sick. And I’m standing right here, and I’m traveling the world and feeling great. That should be enough for you to at least question the medical paradigm a bit.” I will say that probably 20% of people react well to that.
Lindsey:
Yeah, well, in my health coaching training, they had an expression, which is that you can’t save the people who are swimming away from you. So if you have a drowning person, they have to be working in your direction. You can’t chase them down. If you want to get help, you can you can take the first steps yourself. I know one of the other things you mentioned when we had talked before the show was about your hair. Can you tell me a little bit about what changed there?
Jordan Powers:
Yeah, so I actually just finished another ebook, I’ll give you the link for that one as well. It’s going to come out this week. When I was doing all this, I was also putting my stepdad on the same diet. He’s not sick with anything, but he did get off statins for a lot of reasons. He questioned everything in his life after that point, and we were doing the same stuff, with the bone broth, and I’m getting better, and he’s feeling better. He wasn’t battling a chronic illness, but just feeling better in general. And I went to his house one day, and I looked at him and I said, “Oh, my God, your hair looks amazing.” He was putting his hand through it. And it was probably 20% less gray at that point, too. At the same time, I was experiencing the same thing. I’m not talking about dramatic difference, but I’m talking about even my nails growing faster. I would just have filled in my hairline. It was easier also toc lean it, wash it, style it. And so I started looking into that aspect of healing. And it’s like your skin and your hair are the barometer, right? You look at yourself, and you can look at a person and see that they look healthy, even if you don’t know why. Whether it’s the whites of their eyes, or whatever it is.
I put together this book, and I looked into history and you look at photos from the 1900s. It kind of similar to when you look at photos of the 60s and 70s, people on the beach, you see that like 5% of the people are fat. In these photos from the 1920s you see the difference then and I was looking at these guys, they were in their 30s and 40s. Most of them didn’t have receding hairlines. And so I started looking into whether it was getting worse. If we know chronic diseases are getting worse, is balding getting worse too? It was really bad in Asia, people were balding at 18. So I put together this book looking into the chemicals you put in your hair, the sulfates, there’s multiple class action lawsuits now against shampoo makers, some of them probably have merit, and some of them are a cash grab. But I’m of the belief that when you mess with the microbiome of the scalp, you’re going to run into problems. I went into what I do for my hair, basically an organic shampoo bar and some coconut oil. That’s basically it. And then really breaking down more the hormones, raising prolactin, estrogen, seed oils, and the different things that can mess up your hair and linking that information to different studies about filtering your shower water, because I noticed my stepdad and I were going through that. There are also a couple helpful Chinese herbs that people are using and rosemary oil is shown to be as good as Rogaine now.
Some of the more heterodox beliefs, including that a lot of what’s going on is not related to DHT. It’s related to inflammation in the scalp. Why do you never lose hair here, but you lose it here? That’s why they do hair transplants from the back, investigating what’s going on there. I include little bit about blood flow and facial development. And so I put that together and I called it “How not to go bald: 30 all-natural solutions for hair retention.” It’s not a cure all, but it’s all interrelated. Looking at your hair, and why you’re losing your hair at 18 years old, maybe it’s because you’re consuming high amounts of PUFAs. It also looks at parts of the world like the Blue Zones. When I went to Costa Rica, that was another thing I noticed. I couldn’t believe how healthy the people looked because I was near one of the Blue Zones. You’re talking about people in their 70s and 80s and they’re moving boulders and logs. And they’re not doing NAD drips, they’re just living their life. The community is socially cohesive, and they’re living in tune with the earth and staying active. These guys, they’re 70. They’ve got muscles and a full head of hair. I do think it’s all interrelated. I think some people are more susceptible to hair loss genetically, but I put that together and tied it in with what I learned in the book as well.
Lindsey:
One of the things that I thought you’d mentioned initially was about a copper deficiency and the gray hair.
Jordan Powers:
Yeah, that was one of my holistic friends, who recommended taking copper with zinc on a daily basis and see if you can reverse some of the grays. And I would say I probably reversed them like 20 to 30%. So far, it’s been mostly the greys on the sides of my head. I don’t think I’m going to win that battle entirely, but it helps. There’s some interesting stuff now about hydrogen peroxide and how if you lower those levels, you can stave off the gray hair, which I didn’t dive into too much in the book. It’s just so crazy to see my step-dad looking like he has the same the hair he did when he was 35. And he’s 68. It’s strange to see all these things happen, and his skin looks great. I just wonder how much of the stuff we consume normally is being poisoned to a degree.
Lindsey:
I think some people also have poor detoxification, just genetically. I’m going to have somebody on my podcast from a DNA company soon, and I’ve got my reports, and I found out that I don’t naturally detoxify well, so I’ll probably do well to supplement with glutathione or NAC or some precursors to glutathione. That’s something that just genetically I’m burdened with. So that may be you, maybe you are not going to methylate well, you’re not going to detoxify well. There may be things that you will always need to supplement. A lot of people need B vitamins who come into my practice. I think there’s just different ways that our bodies relate to the world.
Jordan Powers:
Well, I’ve always loved niacin flushes. And I’ve done them for a really long time. I’m talking years before, I would do them because some holistic podcast had said they were good for mental health purposes, and this is when I was really struggling mentally. It’s because it opens up the blood flow to your brain, and so you get like a fresh flush like you would when you’re exercising. And so when I was doing those, my mood would do a 180 on a really bad day. I’ve continued doing those for my skin and hair. I hope you’re not going to tell me that they’re bad for you. Because I do them at least once a week.
Lindsey:
No, no. There’s forms of niacin that cause flushing when you take them and there’s forms that do not. You’ll see it advertised as no-flush niacin. I have heard about using niacin for depression. So what kind of doses would you would you take?
Jordan Powers:
I did about 1000 milligrams. So two of the tablets. I get the flushing kind.
Lindsey:
Some people don’t like the flushing feeling. But I think the one that works for depression is the flushing kind.
Jordan Powers:
I believe it increases your NAD levels. I think that’s also one of the other things.
Lindsey:
It’s certainly a precursor.
Jordan Powers:
So I do that because I don’t mind the flushing, I combine it with some sauna, which I find is nice. But little things like that. I’m half Italian, but I’m also half Irish, and the chemical sunscreens really scare me after my discussions with certain people. What I do now is that I don’t go out during peak hours, but I take astaxanthin*, which is that really powerful antioxidant, which is also great for my colitis. When I went to the Caribbean, I was in Anguilla for about six days. And I didn’t go out during the peak hours. So I’d go out from 2-5 pm, no sunscreen, just zinc oxide on my face, but no sunscreen on my body. I would take the astaxanthin. I loaded it about two weeks before, and I didn’t burn once, which is very strange for me. It’s also the seed oil consumption, people believe it’s oxidizing. When I would go to places as a kid, I burned if I went in the sun without sunscreen. In the Caribbean, I didn’t because they say astaxanthin acts as an internal sunscreen. That tip really has changed things for me, because for people that are fair and don’t want to slather on a bunch of chemicals on their skin, it’s a nice option, and you also get the antioxidant benefit of it as well.
Lindsey:
Awesome. Any additional thoughts on things that you’re doing to protect your health right now or things that you’re doing other than the eliminating toxins and an elimination diet that you might recommend for someone with colitis?
Jordan Powers:
I think largely we’ve covered most of them. I will say also the other aspect we haven’t touched on which is a big part of me getting healthier is the mental aspect. It’s one thing to feel better and be able to tackle these things because you’re in a better state of mind. But I’ve started following people like Teal Swan, who’s quite controversial, but she really helped me. I read one of her books. I’ve just been practicing a level of radical responsibility. The idea that I don’t whine about how other people treat me because I can’t control that. Instead I deal with why I stayed. And why I tolerated that behavior and my self esteem levels and what I will tolerate moving forward. That radical honesty and responsibility has really changed my life, and filled it with purpose. Now I don’t get sucked into people’s problems and their gaslighting.
That was a real problem for me that I think was also really throwing off my microbiome. The way I approach the world is I don’t get triggered by people. People can say things about me, and if I don’t believe those things to be true about myself, because I know myself and I have a strong self concept, I no longer react in the crazy way I used to do. Because I can go no, that’s not who I am, and that’s not what I believe in, you’re mischaracterizing me. A lot of this is just a level of maturity, and investing hours into understanding yourself and who you are, and your background. I think that was the final piece of this puzzle to get me to a place where I could look at myself in the mirror and feel good about who I’d become. One of the guys on YouTube, The Heal Your Gut Guy is his name, he spends a lot of time connecting people’s stress and their mental problems with their gut and making connections between the two.
Lindsey:
Usually one of three things I’ve identified that throws people’s guts off is either an episode of food poisoning, a lot of antibiotics, or other medications like steroids, or an extreme period of stress. Inevitably, that starts the whole process of a downhill slide for everybody. So of course, getting the stress piece under wraps is important.
Jordan Powers:
Yes, talking about stress, I do a million things. I have three businesses, I do a podcast, and now I’m deciding to do music. I’m just trying to fill my life with different things and give myself direction. I’m writing a song right now called Cleaning House. The idea behind it is why do I feel like life makes more sense when I get rid of certain people. What comes with that is a level of loneliness; it’s sort of like a tax you have to pay. The idea is that once I once I get rid of 90% of people, I will be happier and have a level of peace. I also will trade that with a bit of loneliness at times, and it’s hard to navigate that sometimes. That’s been a big thing for me is getting rid of people that didn’t serve me and didn’t serve my purpose. I think so many people hold on to people as they get older, because that’s just what you do. But often, it’s not that you’ve evolved past them in a better way, but you’re just on a different journey. You just feel that divergence. I’ve let some people go out of my life that I really needed to let go of for a really long time. I do it in a different way than I used to do it when I was all messed up in my gut. I just have an honest conversation. It’s not about me saying to people, you need to change and you need to do this. It’s about me saying that this is what I need out of our relationship, and if you can’t provide that to me, then I need to do what’s in my control and leave.
Lindsey:
That’s a very courageous thing to do. So congratulations on making that big step.
Jordan Powers:
I think it’s needed for so many people.
Lindsey:
Well, thank you so much for sharing about your journey and the stuff that you’ve been going through. Tell me the name of your two books.
I don’t think most of the people listening are interested in marketing help, but you never know.
Jordan Powers:
Yes, but that’s this is the main thing. Those are the only health books that I’m going to do. This is just something that I’ve gotten into.
Lindsey:
It’s a side passion, right?
Jordan Powers:
I ran into so many people asking me over and over how I cured my colitis. And so I decided, let me just sit down and put it into an ebook and then for the rest of my life, I can just send people the link, and they can look into it themselves. Because people come to me for help a lot, and it’s a lot of time and I also don’t have the training to unravel all their issues.
Lindsey:
Yes of course. People’s health situations are very complex and require a lot of background information and study.
Jordan Powers:
I’m sure you get people that say this to you all the time. They’ll say their health problem is they feel tired, and that could be 500 things. I don’t know how to attack that.
Lindsey:
Absolutely. Okay, well, thanks so much, Jordan. It’s been a pleasure.
Jordan Powers:
I appreciate you having me on. This has been really great. Thank you.
Ifyou’re struggling with bloating, constipation, diarrhea, soft stool, acid reflux, IBS, IBD or any type of chronic disease, etc. and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me (Lindsey). We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
1. Detoxes and cleanses are the ultimate gut health solution or weight loss solution
I’m sure you’ve seen advertised gut detox kits or cleanse plans on the internet that claim they can remove toxins in your gut, or billed as the ultimate solution to a gut health problem, or the best way to lose weight quickly. The gut detox kits might have herbs, fiber, probiotics, something laxative perhaps. Cleanses may be restrictive diets with particular foods emphasized each day or come in kit form as well.
If you were considering a detox kit or cleanse for weight loss, the benefits will likely be short-lived as most of these cleanses are not sustainable in the long-term. While some studies report short-term benefits like weight loss and improved insulin sensitivity, there is insufficient compelling evidence to support the use of “detox” diets for long-term weight management or toxin removal. Even worse, these cleansing diets may lead to temporary weight loss due to reduced calorie intake but often result in weight gain when normal eating habits are resumed. The main consideration for me when it comes to weight loss is that whatever method you’d like to use to lose weight and maintain weight loss needs to be sustainable. That’s why, for example, I rarely recommend a ketogenic diet, because I’ve never met anyone who could sustain that in the long term, not to mention I’ve met several people, including myself, who have had bad reactions and gallbladder issues from such a high fat diet. In one case, I had a friend end up with a gallbladder removal after trying keto, but more commonly, as was the case for me, shooting pains likely indicative of gallbladder issues after following a keto diet for a short time. Of course there are people who can and do sustain keto long-term, but most people crave carbs too badly and eventually come off of it onto a plan that’s much less healthy. So I’m an advocate of starting with something sustainable and losing weight gradually in a way you’re willing to live with for the rest of your life.
Another consideration with a sudden detox or cleanse is a die-off or Herxiemer reaction, especially if you have a very poor diet to begin with full of sugar and processed foods. It’s actually better to gradually go off these types of foods so that as your body starts to detoxify from them naturally, you don’t have headaches, a flu-like feeling or other die-off reactions. A gradual elimination diet with a scheduled reintroduction, like the autoimmune paleo diet, is a better choice if you’re trying to determine whether you have food sensitivities, or trying to stop what seem like autoimmune symptoms or general ill health.
As for gut detox kits or supplements, there was a double-blind, placebo controlled study on one detox supplement containing a 1350 mg blend of papaya leaf, cascara sagrada bark, slippery elm bark, peppermint leaf, red raspberry leaf, fenugreek seed, ginger root, and senna leaf. Participants took it for 4 weeks. The study concluded that “No beneficial or harmful effects of supplementation were found for body composition, waist circumference, gastrointestinal symptoms, or blood markers.” If I had to dig in on why there were no changes, just looking at the ingredients and the dosage, I’d say this. Some of those ingredients individually I know are successful in helping with gut issues. For example, senna leaf teas are well known for helping with large intestine motility for constipation, ginger root is helpful with small intestine motility, and is often included in prokinetic agents for SIBO, and peppermint leaf is known to be helpful with bloating and IBS/SIBO symptoms and slippery elm is good in the case of gastritis and healing the lining of the stomach and small intestine. But each ingredient has a particular best dosage, use and function and just throwing everything into one detox kit no matter what your issue is will not likely produce the desired results. In this study, also, participants were healthy, so it wasn’t looking at the product’s results on people with a particular condition.
But in most cases, gut detox kits or programs will have a limited duration like a week to ten days, and the needed duration for, for example herbal supplements to kill off gut pathogens, may be 4-6 weeks. Or if you’re dealing with well-entrenched systemic candida, you may be looking at 8 months’ worth of treatments, switching active agents every couple months to prevent resistance.
Now there are some higher quality kits, say for example, Microbiome Labs Total Gut Restoration – Kit 2*, but again, they’re for particular situations. I would recommend a kit and plan like that for dysbiosis, but not for SIBO, because at week 5 you’re already introducing prebiotics including FOS that would feed the bacteria that cause SIBO. But most people choosing these kits haven’t done a stool test or SIBO breath test and aren’t quite sure what they’re using the kit to deal with. You could have bloating, for example, from SIBO, from candida overgrowth, or from low stomach acid, among other things. So there’s not really a one-size fits all solution you can just grab in a kit.
Also, when it comes to detoxification, the body does a pretty good job expelling toxins on its own with natural mechanisms, through the lymph system, the liver and kidneys, skin, lungs and digestive system. Of course some people do have markers on an Organic Acids Test* or NutrEval Test* that indicate that they aren’t detoxing well, such has high pyroglutamic or low glutathione, or elevated markers for some environmental pollutants. In that case, I’d likely recommend N-acetyl-cysteine or NAC* or glycine, if certain gut health markers are out of whack, as they are precursors to glutathione, but that’s with specific evidence of liver overload or dysfunction.
The average person doesn’t need a detox kit, they just need to gradually move towards a healthy lifestyle and maintain it through regular exercise, a well-balanced Mediterranean style diet, physical activity, stress management, good sleep, stopping smoking and reducing alcohol consumption. In place of detoxes, short-term fasting or elimination diets can be considered for resetting the gut and promoting healing, particularly when dealing with food sensitivities, autoimmunity, chronic gut issues, or symptom flare-ups.
2. Drinking at all with meals will dilute your stomach acid too much
So I’ve had a lot of guests on my show talking about not drinking with meals, and if you’re anything like me, you would choke if you didn’t have liquids for washing down your food. So I wanted to check the veracity of this claim.
What I found was a study in which participants drank a full glass of water, then they tested stomach pH. Now optimal stomach pH is quite acidic at 1.5-3.5 and but to digest protein properly, you’ll want a pH in the 1.5-2.2 range. Just a reminder from high school chemistry, a low pH is more acidic, a high pH is more alkaline.
So in the study, a glass of water, and water is around 7 in pH, did in fact increase stomach to a pH of 4 for 3 minutes. So if you extrapolate that a bit, it’s hard to image that small sips of water in between bites of food are going to significantly increase pH for any reasonable amount of time. However, I could see some value in pausing between sips of water and more food to allow the stomach to reacidify. But this idea of going completely without liquid seems a bit over the top to me.
3. Popping a probiotic will fix your gut health issues
Probiotics are live beneficial bacteria that people can take as supplements or naturally digest by eating certain foods such as kimchi, yogurt, kefir, kombucha, sauerkraut and other fermented foods. The idea is that by taking probiotics you can rebalance your gut by increasing the levels of beneficial bacteria and limiting the amount of harmful bacteria. They have grown extremely popular recently, and many supplements, drinks and foods include the tiny organisms. Most of these forms of probiotic supplements include the Lactobacillus and Bifidobacterium genera. Despite the craze surrounding probiotics, it’s been difficult for consumers to understand the inconsistencies in claims between scientific studies and supplement companies’ advertisements. It is hard to take in all of this marketing information and reasonably determine the effectiveness of various probiotics and what specific benefits they provide and in what situations.
This confusion happens because there is actually an incredible diversity in types of probiotics, and each of these types of probiotics works differently and on different health conditions. There is no standard probiotic, a fact that the natural health industry often overlooks when marketing and selling probiotic products. This presentation implies that all the microorganisms are homogeneously beneficial, and perpetuates the myth that simply popping any probiotic will automatically help with any health and in particular gut health condition. As convenient as this would be, it’s unfortunately not the case. Probiotics require a precision approach that pays attention to scientific and medical studies in order to figure out what the right choice of probiotic is to address specific issues.
When I suggest probiotics to clients, it’s always specific to their condition, and I often recommend either a probiotic yeast, Saccromyces Boulardii*, that has been well studied with specific conditions like H pylori, for instance, or a spore-based probiotic* that has been studied for reshaping the gut microbiome in a beneficial manner and in particular with SIBO, or a very specific strain of a lactobacillus probiotic for their particular condition. The means not just Lactobacillus reteuri, for example, but Lactobacillus reteuri DSM 19738, which is the name including the genus, species and strain name. Or more recently, now that we have some anaerobic strains available, I might recommend a probiotic like Akkermansia Muciniphila*, for people whose Akkermansia is showing up as below detectable levels on a stool test. But I almost never randomly grab a multi-strain lacto/bifido probiotic as a cure-all for all clients.
And a 2018 study in Cell using multiple stool samples using the best technology available for categorizing the bacteria in stool, called metagenomic sequencing, plus analysis of two samples taken via endoscopy, found that probiotics taken with antibiotics deeply delayed and perturbed the reconstitution of a normal gut microbiome in healthy individuals. But again, keep in mind that the starting point was a healthy gut microbiome, so this doesn’t necessarily apply to dysbiotic microbiota. Lucy Mailing does an in-depth analysis of this study and the pushback from some people in the gut health community if you want to dig further in, but her recommendation is protecting gut hypoxia, meaning an oxygen-free colon, by using butyrate supplements while taking antibiotics if you have a healthy microbiome to start.
And if you’re looking for specific probiotic recommendations, I have a blog I update periodically called “Choosing the Right Probiotic to Heal What Ails You” that you can consult for more specific condition-related recommendations.
4. A gluten-free diet is necessary for optimal gut health
So this is a topic that I’ve done podcasts about, and I have recommended that if you’re struggling with gut health issues, you should try going off gluten. But it’s certainly not a magical ticket to perfect gut health and often, once gut healing is finished, going back on gluten is totally possible and not harmful. Now of course if you’re diagnosed with Celiac disease or non-celiac gluten sensitivity, you should legitimately plan to avoid gluten for life, and that fact will be reinforced every time you eat gluten and feel miserable, if you first eliminate it strictly. Celiac disease is an autoimmune disorder that results in intestinal damage from eating gluten and is effectively managed by strictly avoiding gluten. I should add that I know there are lots of people out there and who I’ve seen as clients who have celiac that’s undiagnosed because they went off gluten, felt better, and never took the test while on gluten. So if you suspect celiac, it’s best to take the test while you’re still eating gluten. While you can test for the genetic pre-disposition for celiac at any time, testing for antibodies (Tissue Transglutaminase IgA antibody being the typical first line test) is best done while eating gluten. Gluten sensitivity, while associated with some gastrointestinal symptoms, lacks specific evidence of intestinal damage. However, for sensitive individuals, there is an extended opening of the tight junctions between cells in the intestines, meaning a leaky gut, which is a precondition for autoimmune disease. So if you’re experiencing any active autoimmune disease, you should avoid gluten. But for the remainder of people, any improvement experienced when avoiding gluten may be related to the fact that wheat is a FODMAP food, which is a type of fiber that is fermented by gut bacteria and produces bloating, or simply because gluten is a large, hard to digest protein and if your digestion is impaired, any more complex proteins may cause you issues.
All this to say that if you do go off gluten while dealing with gut health issues, unless you got a stool or other test indicating sensitivity. And I do see a good number of people, even people who are supposedly gluten-free, who have elevated anti-gliadin IgA antibodies on the GI Map Test*. But if you have no solid evidence of a sensitivity, then you can safely try gluten again once your gut health issues are resolved. I myself, while I was actively dealing with elevated antibodies for Hashimoto’s thyroiditis, went off gluten for years. But I have slowly reintroduced high quality gluten-based breads more and more, but mind you, only ones that have had a complete rise which eliminates most gluten, and after many years of my Hashimoto’s antibodies testing in the normal range. But I don’t go crazy with it because bread is a FODMAP and as someone with autoimmune IBS that causes SIBO to recur, I bloat when I eat too many FODMAPs.
But for those who don’t have recurrent SIBO or a known gluten sensitivity, it’s worth reintroducing high quality whole grain bread products. This is because lots of gluten-free foods lack essential nutrients like folic acid and iron, or they contain less fiber, and may be higher in sugar and fat compared to their gluten-containing counterparts, or are dominated by white rice flour, opening up the possibility of arsenic toxicity, due to the high levels of arsenic in certain types of rice. But just a quick note to say that I was worried about the whole arsenic in rice thing for a while and consequently made a real effort to not use rice flour in my gluten-free baking, but rather use a mixture of millet, sorghum, cassava, oat flour and tapioca starch in my homemade gluten-free flour, and just use some high quality gluten-free bread products from Food for Life and rice/corn chips like the Lundberg ones and only occasional rice flour based products from a local bakery. And then I was eating primarily white jasmine rice at the time. And when I did a hair mineral analysis a number of months back, I had no arsenic show up at all. But anyway, the idea that gluten-free diets are universally more nutritious or prevent disease has not been scientifically proven, so it’s important to figure out what is a genuine medical condition or sensitivity before making a final decision on gluten.
5. A healthy gut is solely determined by diet
I have a lot of clients who doggedly pursue dietary changes from paleo to keto to carnivore to fasting to long-term low FODMAPs or low-oxalate or low-histamine diets or some combo thereof in an effort to improve their gut health. And in the course of this, I find that they can get in a dangerous downward spiral quickly where their body is used to so few foods, they react to almost everything. While I definitely approve of advocating for yourself and trying as much as you can on your own and in assistance of any protocols I might recommend, diet is just one piece of the puzzle when it comes to restoring gut health and maintaining a healthy gut. In many cases with overgrown bacteria or candida, antimicrobial herbs or spore-based probiotics, or serum bovine immunoglobulins may be necessary to eliminate pathogens as well. Then on top of that, various lifestyle and environmental factors also significantly influence your gut microbiota. Habits like smoking and a lack of exercise, for instance, can have a substantial impact on the large bowel and potentially the gut microbiota, increasing the risk of gastritis and colorectal cancer. Stress, through its influence on colonic motor activity via the gut-brain axis and increase in cortisol resulting in increased blood sugar, can alter the gut microbiota, possibly reducing the presence of beneficial bacteria and contributing to IBS-like symptoms. Underlying health conditions, such as diabetes, prediabetes and autoimmune disorders can further complicate gut health. Beyond lifestyle and health, factors like poor sleep patterns and even travel can also affect gut health. Sleep deprivation has been linked to changes in gut microbiota and increased gut inflammation, while travel, especially to foreign destinations, raises the risk of contracting parasites and bacterial infections that impact gut health. So, while diet is a crucial component of gut health, it’s only one piece of the puzzle. A holistic approach that includes managing stress, getting regular exercise, and considering other factors is essential for promoting and maintaining a healthy gut.
6. The more fiber, the better
While most people who consume a typical western diet don’t get enough fiber, consuming too much fiber in the wrong situation or too quickly can have negative effects on your digestive system and overall health too. While dietary fiber offers several benefits, including improved stool consistency, regularity, digestion, and potential protection against diseases like cardiovascular issues and colon cancer, it’s important to know when and how to introduce added fiber. The recommended adequate Intake for fiber is around 25 grams for adult women and 38 grams for adult men, and ideally this should come from your food, but if you can’t get enough from your food, and decide to take a fiber supplement, you should do it gradually. Even adding fiber via food like beans is ideally done more slowly. Most people know that a sudden intake of beans leads to gas, which is because most people’s microbiota doesn’t have enough of the gas-eating bacteria that feed on the gas produced by the microbes that ferment the beans into gas. So if you’re on a long-term fiber increasing plan, it’s best to start with a tablespoon of beans or lentils, ideally cooked from dry beans, properly soaked and rinsed (and I mention beans and lentils as they’re some of the highest-fiber foods) and work your way up to ½ cup a day or more. And for a fiber supplement, start with a pinch and work your way up to 5 or 7 grams a day. Rapidly upping your fiber intake can lead to gastrointestinal discomfort, as the bacteria in your gut may digest the excess fiber, resulting in gas, bloating, cramps, and abdominal pain. Or for people with constipation, excess fiber may stop you up even more if you don’t pick the right one or haven’t done other things to promote motility first. Moreover, excessive fiber can hinder calcium absorption, potentially causing more harm than good, so you’ll want to take that excess fiber away from supplements and meals. Promoting unrestricted fiber consumption as a strategy for appetite suppression, fullness, and weight loss is not a healthy approach. Balancing your fiber intake and gradually increasing it in line with your individual needs, conditions and tolerance is the key to reaping its benefits without adverse side effects. And if you want more info on fiber types, I did a whole episode on fiber in episode 96, which I’ll link in the show notes.
So that’s the six gut health myths for today. As always, if you want some professional help, I work with clients with gut and all over chronic health issues. So ifyou’re struggling with bloating, constipation, diarrhea, soft stool, acid reflux, IBS, IBD or any type of chronic disease, etc. and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me (Lindsey). We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
As featured on Feedspot as #18 in gut health blogs!
Adapted from episode 107 of The Perfect Stool podcast hosted by Lindsey Parsons, EdD, Gut Health Coach and edited for readabilitywith Dr. Loredana Shapson, PharmD, FNTP, founder of LifeMod Solutions, a holistic health practice in Newtown, PA.
Lindsey:
So why don’t we start with your gut health story? I know your history involves taking a lot of antibiotics, much like mine and many of my listeners.
Loredana Shapson:
Yeah. Which ended up taking a turn for the worse after that course. So I suffered from constipation for most of my life since I was a teenager. I would only go to the bathroom maybe once or twice a week. If I did, it was not very satisfying. It was small, little pebbles, nothing. Then eventually, as I got older, I started to bloat and it would happen randomly and unpredictably, with certain foods and sometimes not others. Like anybody else, I started to look on the internet. What’s causing my bloating? What could this be? I started putting myself on supplements, and I started working with a couple of gut specialists. Even after working with some of these people, and doing a lot of stool tests, and SIBO tests, and all of that, I still wasn’t getting some of the results that I had desired. But I’d spent a lot of money seeing some of these people.
Eventually I got put on an antibiotic. After I got put on that antibiotic, my gut symptoms actually got worse, not better. So when before I was bloating randomly, it was now happening every single day. When I would wake up in the morning, I would have a flat stomach, and then I would drink water. Then boom, I would look like I was nine months pregnant. It was that drastic. So I had extreme food restrictions, I couldn’t even take a bite of avocado or not even a teaspoon of fermented food, no liquid, nothing. I was so triggered by all that. When I had my bloating, I also had mood issues, like irritability and anxiety and focus issues. I couldn’t sleep very well, I had trouble losing weight. I was just realizing that my gut is connected to my entire body and affects all other parts of my body.
With my background in pharmacy, I eventually researched how to fix gut health. I found some shortcuts. Now I’m using everything that I did with myself with my patients. I’ve been treating patients for about two years now, specifically for gut health and for that particular focus. It’s been really awesome to see the increased healing, the less supplements that are needed, the more food they can bring back in sooner. It’s exciting to be here on this podcast. I’m happy to be on your show today to share some helpful tips for your listeners.
Lindsey:
Yeah, that’s awesome. So did you figure out it was SIBO in your case? Was it methane SIBO? What was going on?
Loredana Shapson:
Yeah, so I did take a SIBO breath test. It was both. I had a mixture of everything. I had four stool tests over the course of two years. And the stool tests didn’t really provide much data for me. I mean, it did show that inflammatory markers were up, but obviously if your gut’s imbalanced, your inflammation is going to be up as well. So it showed dysbiosis. But it didn’t really change the way that my functional medicine doctor at the time was was going to go after helping me. But yeah, it was methane SIBO and I just remember spending a lot of money on supplements. I think at one point I was on like 18 different things. It was crazy.
Lindsey:
I can believe it. So we did agree to focus on bloating in this episode. And that’s, I guess, where you’ve started focusing your practice. So talk to me about the different causes of bloating.
Loredana Shapson:
I like to funnel bloating into two sections. So first and foremost, it is imbalanced gut bacteria, whether that’s an overgrowth of something and not enough of another. We can have SIBO, which you just mentioned, which is the bacterial overgrowth, and then there’s also SIFO, which is fungal overgrowth. I see a ton of that in my office. And then we also have SIPO, which is parasitic overgrowth. So all of these can be imbalanced from one level to another, and they can cause bloating.
The question is, how do we get an imbalanced gut? I’m sure you’ve talked about this on your podcast before, but it’s antibiotics in prescriptions, antibiotics in our foods, and other prescriptions can cause bloating. There’s also things like the pesticides and herbicides, preservatives, all of these things that kill bugs; chlorine in tap water. All of these things are going to create imbalances in our gut. So that’s first and foremost. And then the secondary part of this picture is low digestive enzyme release. So what causes that? Well, first the gut imbalance can lead to that. The secondary thing is stress. I like to funnel stress into three little tubes where first is physical stress. Say you fell, you had a surgery, whatever it is, your body’s in physical stress, and it’s turning on your sympathetic nervous system, which is your fight or flight response. The next is emotional stress. Maybe you have a really big project at work or you’re fighting with your partner, that emotional stress triggers your fight or flight response. Then the next is chemical stress, which is things like pesticides or herbicides, antibiotics. It could even be heavy metals and the things that are in our personal care products that are causing stress on our body.
And the bottom line here is, whenever your stress is on, and your fight or flight is on, your digestive system turns off, which we call your rest and digest nervous system. So when I approach healing my patients, we got to give the patients digestive enzymes now, because they’re not making enough right now, whatever their cause is, it doesn’t matter, we want you to feel good. So digestive enzymes come first. And then we work on imbalance in the gut, which has to do with your diet, supplements, and probiotics, so on and so forth.
Lindsey:
So how do you approach testing in your patients? Are you running stool tests and seeing their enzymes are low?
Loredana Shapson:
No. So I actually don’t run any stool tests on any of my patients, and I’m still getting pretty awesome results. And so the reason why I do that is because the clinical research is showing that, yes, stool tests are great in clinical research because they’re understanding what therapies do and how it affects the gut microbiome. But I want to bring up one particular study, it was a meta analysis. Meta analysis for those of you that don’t know is almost like the second best type of research that you can use to apply to patients compared to randomized clinical controlled trials. There was a study done in 2019. This was a meta analysis that included 11 trials, and it had over 729 patients. And what they wanted to look at was “Do prebiotics help IBS symptoms?” They compared prebiotics users to a placebo group. I know we’re not talking about prebiotics right now, but it was interesting in this study that they looked at stool tests from patients before and after.
When they looked at the study results, prebiotics did not improve GI symptoms, it didn’t improve quality of life, it didn’t improve functional bowel disorders, it didn’t improve bloating, or gas or abdominal pain. What they did see was in the stool tests that the Bifido group did grow. So even though the stool test looked a little bit better from when they got started, it still didn’t equate to the patient feeling better symptomatically. So that’s one study that really stood out to me to say that we need to step away sometimes from taking all of these stool tests, and all of this lab work and focusing on the numbers for patients. What I particularly focus on is how do you feel? Are you getting better? Is your bloating going down? Those are more of what I focus on in a lot of my patients.
There was another study done in SIBO patients where they did a SIBO breath test. They wanted to see if they could use a SIBO test to determine how they would respond to a low FODMAP diet. After this study, what they found was it wasn’t the levels of methane or hydrogen that really determine the response rates. What determined whether somebody was going to do well on a low FODMAP diet was their symptoms at the time that they were started. The more severe symptoms they had, the better that they would respond to a low FODMAP diet. So that was an interesting kind of a study too, because it shows us that the test, even though it’s positive, doesn’t always show that they’re going to feel a certain way.
Lindsey:
What about H. pylori? I mean, that’s one where I really like to know about when I go into working with someone. Without a test you can’t know if they have it or if it’s overgrown.
Loredana Shapson:
So H. pylori is definitely something that I haven’t had to test here in my office. I would like to know if my patients have had the test done with their GI doctors, because that does change things a little bit because H. pylori can cause ulcers. One thing that I ask my patients whenever I think H. pylori is an issue for them is: are you having pain? Is it really harmful? Are you having cramps, and is it really uncomfortable? Another thing that cues me into that is are you taking a Betaine HCl* supplement or an acidic supplement for digestion? If that’s causing you pain when you take it, or even if vinegar bothers your stomach and causes you pain, then maybe you have an ulcer. Maybe that could be from H. Pylori. So that would be a different scenario. I haven’t seen too many H. Pylori patients in my office. But I know that at the end of the day, what we find is that as soon as you come in with the good probiotics, everything starts to rebalance.
Lindsey:
And what about testing for SIBO? And using Organic Acids? Do you do that at all?
Loredana Shapson:
I have. Yeah, that’s probably the test I run the most in my office is the urinary OAT by Great Plains. And I will check that in my patients when they have severe issues if they really want to know. It’s not typically covered by insurance plans, and you’re going to spend at least $300 to $350. So if the patient really wants it at the start, I will give it to them, but otherwise, if we go down this course of taking care of SIFO, usually I’ll pull that urinary test about four to six months in so that we can see how we are doing. Is there still an issue there? We always want those numbers to be in the lower 20th percentile for the markers one through nine.
Lindsey:
So how do you approach treating people with gastrointestinal issues if you’re starting without a test?
Loredana Shapson:
We look at symptoms. I mean, first and foremost, it’s digestive enzymes. That’s key. We start with diet and enzymes to get things moving. So number one, if they’re not pooping, we get them pooping. If they’re having diarrhea, we try to stop their diarrhea because they’re not absorbing their nutrients efficiently. So that’s correction number one is to fix their stool frequency, whether it’s constipation or diarrhea. Usually, once you add a digestive enzyme, it can rebalance on its own. Constipation gets better with digestive enzymes, because you’re breaking down your food better. We find that once you start increasing the acidity of the stomach, that you’re actually already beginning to correct the imbalance of the gut, because stomach acid’s important for killing bad guys that aren’t supposed to be there. It’s why we have stomach acid, because we were bringing in a ton of microbes through our mouth on our food and everything that we’re touching. Once we start increasing the stomach acidity, we’re rebalancing the gut inherently just by doing that. So I usually start with enzymes, and then add either something to help them poop if they’re not pooping, or whatever they need to do to slow down their pooping, if it’s an issue with diarrhea. Once they’re on that for a couple of weeks, then we start thinking about probiotics.
Lindsey:
Are you doing enzymes that have Betaine HCl in them? Or is that separate?
Loredana Shapson:
So we’re doing Betaine HCl separately, and then if they require another enzyme, depending on how severe their bloating is, I’ll add another enzyme that has everything for protein and fats and other carbohydrates and different fibers and cellulose and all those. Generally, I do really well with just a betaine supplement.
Lindsey:
So when you were saying enzymes, really, you’re talking about betaine HCl?
Yeah, generally, betaine is a big fix. If you think about the way the digestive system works, I call it a three legged stool, right? You got your stomach, your pancreas and your gallbladder. And if one of those legs are kicked out, the whole system kind of collapses. But the core of that three legged stool is the stomach, because once you have enough stomach acid, that triggers the pancreas to release appropriately. And then once that happens, the gallbladder releases appropriately as well. So it’s really the stomach acid that determines the next chain of events down below. If you fix stomach acid, you’re automatically going to fix the enzyme release.
Lindsey:
And will you give Betaine HCl to someone who is actively suffering from what seems like reflux?
Loredana Shapson:
Yes, that’s actually what I recommend to patients who have reflux. It’s often a difficult conversation to have, they don’t understand. They’ll say: wait a minute, I have acid reflux, and you want me to add acid? And I say yes. I often tell my patients what you can use in your kitchen is vinegar. I like apple cider vinegar, because it is a probiotic, but any vinegar works, as long as it doesn’t have sugar. Take a tablespoon of vinegar, and one to three ounces of water. Take that down, and then wait at least an hour before you drink any other liquids, because you want that acidity to do its job. But ideally, if you’re feeling acid reflux, you’re not digesting your foods properly and it’s sitting for too long in your belly. It’s pushing that valve open and causing acid reflux and little drops of acid are getting into the esophagus where they shouldn’t be. So you just want to keep things moving downward, which you do with acidity, and, boom, you’re not going to have that problem. So I definitely recommend that to all my patients when they have acid reflux, either use vinegar or betaine, and get rid of it.
Lindsey:
And are you using the vinegar before the meal because you said to not to drink anything else after that?
Loredana Shapson:
Yeah, so you could use vinegar to help with your acid reflux symptoms at that moment. And then also, you can take it at meal time. I’m not particular with taking it at the beginning of the meal, during the meal, or after. As long as it’s with the food, it’s going to do its job. I like to simplify things. One of the things that bothers me about some of the gut health stuff that’s out there is that they make directions very complicated. It has to be an empty stomach, not an empty stomach, before food, one hour before food, an hour after eating. I find that compliance with my patients becomes very difficult at that point. So for me, I don’t care. Take your vinegar before, during or after, either way, the patient always seems to get benefit. And so clinically, I’m seeing that it doesn’t really matter. But obviously everybody’s different. And you have to try for yourself to see what works for you and your patients. I mean, do you notice any patterns or trends in your patients who take vinegar before or during or after?
Lindsey:
I usually don’t know that level of detail with my clients. You know, I say that this is something that you take with a meal. Whether they take it at the beginning or the middle of the meal, I don’t know.
Loredana Shapson:
Yeah, so that’s the thing. I hope people can see that it doesn’t have to be as complicated as everyone makes it out to be.
Lindsey:
I was just curious because you said to not drink anything else after. So you’re basically telling people to eat without drinking?
Loredana Shapson:
Oh, yeah. 100%. You don’t want to drink a lot of liquids with your meals because it’s going to dilute your stomach juices. We want to maintain the acidity in our stomach. The more water you’re adding to it, you’re going to slow digestion down. It’s going to increase your risk for bloat. You’re going to feel full with a distended belly. What I always tell my patients is that hydration has to be between meals with room temperature water, about a half hour before you eat or an hour after you eat.
Lindsey:
I find that very challenging. Personally, I take all my supplements with my meals, so I have to drink as I can’t get them down without it.
Loredana Shapson:
You can certainly sip as needed, but you should not be chugging a full glass of water.
Lindsey:
So is there a particular enzyme product you like?
Loredana Shapson:
I like standard process Zypan* because it has betaine in there, but it also has some pancreatic enzymes. So that’s what the Zypan stands for, Zy for enzyme and pan for pancreas. There’s a little bit of pancreatic enzymes in there. Plus some betaine. And there’s also some organ meat tissue in there too, which is really healing. There’s some spleen tissue, and they all help heal the gut.
Lindsey:
And do you do the betaine with the challenge approach where you start with one pill, then increase?
No, I usually find patients do really well with two pills. If they have severe bloating, we’ll do three with each meal. Two seems to be like the magic number. And then once we get probiotics on board, I find that the Zypan dose ends up coming down to one with each meal, and then only as needed if they have acid reflux. Typically at that point, it’s usually not an issue anymore. And then eventually, once the probiotics are on board for a couple of weeks, Zypan falls off. I think the probiotics start coming in, and they start helping you break down your food, you don’t need the enzymes anymore.
Lindsey:
So what kind of probiotics are you using?
Loredana Shapson:
Oh, my favorite one is Megasporebiotic* by Microbiome Labs. They’re my flagship probiotic, it’s so well tolerated in a lot of my patients, because they’re non-histamine forming probiotics. So that’s the one I always start my patients on. And you know, everybody’s a little bit different on the starting dose. I don’t follow the directions on the bottle. I never do that for any of my gut supplements. I always start at a quarter of the dose that’s recommended on the serving size. Anytime you’re doing anything with the gut, slow and steady. So even if it says two capsules, don’t start there. Maybe do one capsule every other day. You’ll be on that for a week, and then you go to one a day. But I find that slow and steady wins the race here. You’re less likely to have those Herxheimer reactions and those negative, sick reactions that most people hate. You lose a patient quickly if they have a bad reaction.
And so if you see someone with diarrhea that’s not clearing up with enzymes and Megaspore, where do you go from there? So at that point, I go to gut inflammation. Biotics research has a product called GI Resolve*. That one includes gut soothing and healing nutrients with N-acetyl D-glucosamine and aloe vera. You’re basically reducing inflammation. Then another product I will try specifically with my patients who have a lot of immune issues, histamine reactions, Crohn’s, or ulcerative colitis is MegaMucosa* by Microbiome Labs. That’s a great one. But I find that the GI Resolve is my go-to and then MegaMucosa is what I’ll bring in a little later. And that usually repairs the gut, I find that two or three days after starting that, diarrhea goes away, and patients start to have more firm stools. And I see that if they have blood in their stool, that goes away as well. So we’re really healing the gut with those nutrients for sealing it, reducing inflammation. That’s going to help with the bowel so you’re not pushing your stool out so quickly.
Lindsey:
So I’m curious, because I just had someone who told me they started GI Resolve, and then their gut felt like it went on fire. And I thought that was odd, because that product is something that’s supposed to heal and seal. What would you make of that?
Loredana Shapson:
My initial instinct is to say that they need a binder. So whatever healing reaction is occurring, they’re probably releasing a lot of trash. And oftentimes, a binder is going to mop up that stuff. So I like GI Detox* by Bio Botanical Research. That’s a pretty good starter binder that you could add, but obviously you have to leave two hours between taking that and any other supplements or food. But that’s my instinct. If something goes awry, you lower the dose to be extremely slow. I’ll start people on that by taking one teaspoon. I always start low and slow, then increase every week. They’ll be on it for six weeks, which is more than they’ll ever need, but it’s still a good way to do it.
Lindsey:
And how do you approach SIFO or Candida?
Loredana Shapson:
Yeah, so SIFO is interesting. I see a lot of that in my office, unfortunately. So what we do there is basically the same starting approach because as we correct the digestive enzymes and the acidity, you’ll start to rebalance the gut. The next thing is you start getting into probiotics, they’re going to start balancing out the SIFO and the fungal overgrowth. Sometimes in most cases, I do have to add in a fungal product, which is an herbal product that gently gets rid of the Candida and the yeast. So my favorite product to start people on is by Systemic Formulas called Fungdx*. It’s a great product that’s really well tolerated. Systemic Formulas tells you to do two pills in the morning and two at night. I don’t do that dose; it’s too high. I find that people have negative reactions from die off. I start people on one a day.
And what I have found is that SIFO requires a long haul kind of approach. I’ve had to care for patients through SIFO for up to eight months. It takes some time to totally be eliminated, unfortunately. It’s a slow and steady process. So the more herbals that you add, you absolutely have to add binders too because of the die off. The mycotoxins that die off releases, in general, are some of the worst. They can cause so many issues from anxiety to weight gain, irritability, bloating. It can cause a lot of problems. So always paired with SIFO, if I ever put an herbal product on, is a binder for the whole time they’re on an herbal product. I find that when I don’t, the patient has Herxheimer reactions, they have bad reactions from it. So one of my favorite binders is by CellCore. They have a binder called Biotoxin Binder* (purchase using patient direct code: I0rdLMOm). And it’s specifically formulated to catch yeast and mold toxins. And so that one is expensive, but worth every penny.
As a case study, I had a 30 year old female in my office and she had sores all over her body, up and down. They would show up as red inflamed, and they would ooze, then they would heal over and scar. So she was embarrassed. Summertime was coming up. She didn’t want to wear shorts. She’d been to a dermatologist. She had been to doctors, and nobody was able to help her. I uncovered in my office that it was an overgrowth of fungus because she had had so many antibiotics since childhood for sinus infections, that fungus overgrew. As soon as I put the biotoxin binder on, all of her sores, new ones stopped opening up, which was a great sign. They just stopped forming. Unfortunately, the ones that scarred over were still there. But just by adding that binder, we saw a huge shift in the amount of new sores that were coming out. So yeah, I can’t rave about that particular product enough when it comes to SIFO. Have you heard of CellCore before? Have you used their products before?
Lindsey:
I have heard of CellCore, but I don’t generally use it. They’re not available through Fullscript. So it’s like you got to send somebody to it separately. Their products are not cheap, too. So that’s an issue. But yeah, I do have access to them and have used them with some people.
Loredana Shapson:
That’s my limitation too with them. They’re a great product line, but they’re too expensive. I only pull those big guns out when I need to.
Lindsey:
Can you dig in a little bit more about that skin-gut connection? People might be asking why those two parts of the body are connected. Is it literally the yeast coming out of the skin?
Loredana Shapson:
It’s a great question. And so whatever’s happening on your skin is a representation of what’s happening in your gut. And this goes for acne, for eczema, not just sores and all of that. But the gut lining and the skin and even your nasal passages, all those mucous membranes are made up of the same cells. They’re responding to the same influences, which is the fungal infection in the gut. I think it’s just an imbalance in the gut. And then yes, you could be releasing mycotoxins from your skin and it’s just coming out as irritation. Anytime you have a skin thing, always think of the gut and once you start rebalancing the gut, the skin always gets better.
Lindsey:
I have had some people with super persistent skin issues like eczema that just keeps coming back. Even through multiple rounds of every possible probiotic, you can imagine, every possible antifungal, antimicrobial, the condition still just keeps coming back.
Loredana Shapson:
Can I dive in a little more? How long have they been on the probiotics?
Lindsey:
Continuously, for years. Probably for a year.
Loredana Shapson:
Okay. And then what products do you use for fungal?
Lindsey:
So a lot of times, you have clients who go off on their own and get their own products. So this patient was using a variety of products, but there was one in particular that was a combo antifungal that had berberine, caprylic acid, undecylenic acid, and grapefruit seed extract, which I try and avoid because I know that that really decimates the microbiome, but that was something that he decided to take on his own.
Loredana Shapson:
Oh, interesting because I use grapefruit seed extract* in my mold patients, but I’m not getting negative results to their health after using it.
Lindsey:
Well, sure, they make people feel better. I just see on the stool reports that after taking grapefruit seed, then their Akkermansia disappears.
Loredana Shapson:
I would say that one thing to look at if their eczema is still coming back is the type of probiotic that they’re using and the quality of it, and how long they’ve been taking it. So that’s a minimum of three months every single day and they should have a blend of the spore-based probiotics. The Lacto-Bifido is going to be even more important than the spore-based ones. And then you have to rotate your SIFO products every two months. You should always be changing your SIFO herbals because of resistance and that kind of thing.
The other thing to think about is the environment. So are they continually exposed to something where they’re living or where they work that exposes them to mold that they are not aware of? I personally went through a mold infection twice with two different exposures, one at work and one living with my in-laws for a little bit when my house was under construction. I noticed it because my gums were bleeding every morning, and it happened like day two of me moving in. I didn’t understand why. Then I started developing anxiety, and I started to have irritability and I just felt completely off. A couple of months in, I found out they had mold in their basement. I’m like a little mold thermometer now. I was able to help my in-laws with that. It takes a long time. I would say try to have the SIFO products rotating every two months for a minimum of eight months, and then checking their environment.
Lindsey:
And would you continue the SIFO products that long for anybody who’s positive? Or is this more in proportion to the numbers that you’re seeing on the test?
Loredana Shapson:
Yeah, I would say numbers on the test is where I go when deciding the length of treatment. But I have seen that eight months is usually my average. So with patients who are struggling with eczema, do you find that you’ve been on up to eight months worth of SIFO supplements?
Lindsey:
At least three months of Megaspore, two per day, and CanXita Remove for at least six to nine months.
Loredana Shapson:
I find a good combo that I like to use is Candida Complex* by Klaire Labs. I do also use grapefruit seed extract twice a day with Candida Complex. I find that that combo works really well.
Lindsey:
It’s powerful. That’s the dilemma, right?
Loredana Shapson:
Yeah, I think that while Akkermansia goes down, I feel like the short term benefit of getting rid of that yeast and mold is more beneficial than worrying about Akkermansia. Because it’s going to be very easy to bring back Akkermansia after the fungus goes away. So I think that the benefits outweigh the risks in this situation. I would use grapeseed. I’m speaking from my clinical experience, too. I’ve had patients do really well on that. But again, I’m also not pulling stool tests like you are to see the difference. But all I know is my patients are feeling better, their pain is going away, their headaches go away, so I would maybe try something different. Another thing I would think about too is a gut healing nutrient again, like GI Resolve. Any of those products just to seal the gut up again.
Lindsey:
The funny thing in this particular case was the thing that would clear this eczema was doxycycline. The patient would keep going back to the doctor and getting doxycycline. So I’m wondering, is it bacterial? Is it not fungal?
Loredana Shapson:
Yeah, interesting.
Lindsey:
It’s tricky. I’m sure you have tricky cases. Everybody does.
Loredana Shapson:
Doxycycline is such a big gun to use, because it’s a broad spectrum antibiotic. So I feel like in the long run that’s making the SIFO go up. That’s not helping in the long term.
Lindsey:
I certainly tried to get him off it, but it’s the only thing that would clear it, and it’s on his face. So of course he’s worried about that.
Loredana Shapson:
Yeah. Then topically, grassfed tallow* is really soothing for skin stuff. So give that a shot to just keep the issue at bay while you’re working on the underlying stuff.
Lindsey:
I’ve never heard of that. That’s interesting.
Loredana Shapson:
Yeah. You have to go back to animals and animal fats.
Lindsey:
So you mentioned Lacto-Bifido probiotics too, which ones do you like there?
Loredana Shapson:
Yeah, so I like Designs for Health Probiomed 50*. So when it comes to probiotics, I’m glad we’re touching on this. It’s really interesting. The question I get is, oh, my gosh, there’s so many probiotics out there. How much do I take? 10 million, 25 billion, 100 billion, there’s all these doses that are out there? Do I take it on an empty stomach? Should it be refrigerated? It’s become this intimidating thing. And here’s the answer. Here’s the summary. It doesn’t matter what the heck you take, just take it every single day. It doesn’t matter, once a day is all you need. And the clinical research is showing that a lot of these meta analyses, when we pull together these trials where we’re studying 4000 patients, 7000 patients, all of these trials, the average dose is about 25 billion. It’s not that high. But the range is from 10 billion up to 100. You’ll see 100 billion in some of the IBD cases, like Crohn’s and Ulcerative Colitis. But still, the average over all of these is about 25. So what I use in my office at the start is Probiomed 50. That is 50 billion. And I find if I use anything higher than that, they get negative reactions. So I avoid that.
Lindsey:
And that’s a combo Lacto/Bifido, multi-strain kind of affair?
Loredana Shapson:
Yeah.
Lindsey:
And does it have streptococcus strains in there?
Loredana Shapson:
No, I avoid streptococcus and I actually avoid Saccharomyces boulardii as well.
Lindsey:
It’s so funny about this; there’s people who love Saccharomyces boulardii and people who hate it.
Loredana Shapson:
Yeah, yeah, I know. It’s like a catch-22. I don’t like it because of the urinary tests that I’ve run. I’ve also run some food sensitivity panels on some of my patients and a lot of them show antibodies against Saccharomyces. So I try to avoid more fungal stuff; that’s a fungal strain. And so the body doesn’t want fungus right now. And I find that 100% of my patients are overgrown with fungus because of the way we live our lives and the diets that we eat, high in sugar and refined carbs, and antibiotics and environmental exposures as well. So I really just focus on the Bifido and Lacto, and the Bacillus, the spore-based species, and I get really good results. And after that, eventually, a couple months in, we’ll start adding fiber supplements and that’ll help also with the growth of the good bacteria as well.
Lindsey:
Okay, so not prebiotics, but fiber in particular.
Loredana Shapson:
Yeah, like in the beginning, I’ll start with soluble fiber. There are basically two types of prebiotics, there’s the insulin type, which is like your FOS, the fructans and the galactooligosaccharides, the GOS. Those can cause bloating; they’re fermentable. I mean, that’s just what they are. They’re the inulin type. The others are non-inulin types. So these are things like guar gum and pectin, and these are the ones that won’t cause bloating, the 2′-FL.
Lindsey:
The HMOs.
Loredana Shapson:
Yes, exactly. Yep. So the human milk oligosaccharides. And so they’re not fermentable, they don’t cause gas or bloating. So I’ll usually start my patients with fiber like that first, after they’ve been on the two probiotic types for at least a month or two. And then we’ll start bringing in some fiber. And again, that study I brought up earlier in this conversation, that was the study that really was like, wow, prebiotics are not the fix when you try to feel better. Now when it comes to IBS and bloating and abdominal pain.
Lindsey:
Well, yeah no, the last thing you need to do is add more food for . . .
Loredana Shapson:
Yeah, exactly. So we do that later on, once the good guys are back in. So yeah, my favorite product to start, which is really well tolerated, is by Thorne Research, and that one’s Fibermend*. My patients do really well with that at the start. But again, the directions are for one scoop. I never start there, I go to one quarter of it. And then we stay there for a week or two. And then we go up a little bit. Here’s another thing to a lot of the research with prebiotics and fiber; the doses that they’re using, the average dose is about five grams. So when you look at some of these fiber products, one scoop is sometimes 11 grams per serving; that’s too much. So we’re even seeing in clinical research, less is better. It’s a slow and steady thing. So where do you max out then? So that usually I’ll usually keep people at a half a scoop, but I have more people up to one, it takes about a month to get there. But we’ll get to one scoop and we stay there for a little bit. And then eventually I’ll add MegaPre.
Lindsey:
And if they take more, then they end up getting bloated again?
Loredana Shapson:
Yeah, like sometimes they’ll just have a negative reaction. So everyone’s a little bit different with how they respond. But obviously they don’t feel well. So okay, that was too much. Go back to what you were doing. We’re going to stay there for two more weeks, and then we’ll increase after that. Yeah, like think of your gut, like I tell my patients, it’s like you’re working a muscle out at the gym, you’re not going to go into the gym lifting a 50 pound pearl weight right away, you’re going to start at five pounds, you’ll start at 10. And then after a couple of weeks, you go a little more, you go a little more, your gut’s the same exact way.
Lindsey:
So without doing stool testing, how would you approach parasites?
Loredana Shapson:
Parasites, I usually uncover in the other testing that I do in my office, which is the muscle testing.
Lindsey:
Okay, we haven’t talked about it on the show. I’m not big on muscle testing. But go ahead and just tell me what you do to determine if someone has parasites?
Loredana Shapson:
Yeah, sure. So I do something in my office called muscle testing. And it’s taught by chiropractors, the science of Applied Kinesiology. But basically, I put things near your body, and using the strength and the weakness of your muscle, it tells me whether your body likes it, or doesn’t like it. Is it something I want to talk about or not talk about? And so the reason why we’re able to do this is because we have this energy field that comes out around our body. We cannot see it, just like we can’t see our phones talking or the oxygen that we’re breathing. But we know it’s there. It’s this nice big bubble. And you know, people can take a picture of it. Some people call it your aura, whatever you want to call it. That’s in the medical literature. It’s called the biofield or the morphogenic field.
So when I’m putting things near your body, now it’s making an assessment “Do I like this or not”? Or is it significant to me? And so in my office, I have parasite vials and it has the digital imprint of what a parasite’s frequency is, what it vibrates at. So we’re energetic beings. Everything around us is vibrating. Everything in the universe has a unique frequency down to its decimal point, you can actually measure it, just like every human has a unique fingerprint. So aluminum vibrates at a particular frequency, mercury is different. So parasites are also different. They’re their own little living beings. And so in my office, I have parasite vials for flukes, amoebas, egg layers and non egg layers.
Lindsey:
Like live parasites?
Loredana Shapson:
No, it’s just the digital imprints in water. So it’s a vile, they have found that water has a memory, just like a computer system. So it’s for lack of a better word like electrified water, but it’s containing that digital frequency. So when I bring the parasitic frequency into your energy field, your body tells me whether this is significant or not. And if it shows up, then I know that they’re dealing with parasites. And that’s how I start my parasite protocol.
Lindsey:
If they’re weak in response to a parasite, does that mean they’ve got it or if they’re strong?
Loredana Shapson:
Depends on the test that you’re running. Generally, weakness is what is going to say like, yep, this makes me weak right now, this is an issue.
Lindsey:
Yeah, no, that’s something I’ve just sort of stayed away from because I don’t understand or necessarily know about the science behind it. I’m open to anything that’s got peer reviewed research.
Loredana Shapson:
Yes. And this does. I’ve got three studies I can send you about muscle testing. And it’s been paramount in the way that I approach my patients and it reduces Herxheimer reactions and helps me individualize nutritional supplements too.
Lindsey:
We sort of discussed it, but if you wanted to summarize, is there a treatment order you follow in terms of things like parasites, yeast, bacteria, etc.
Loredana Shapson:
When it comes to patients with bloating, I generally start with the enzymes and the probiotics. I used to go right in with an herbal product like Dysbiocide* or FC-Cidal* by Biotics Research and more herbals, and I really stepped away from that, because I went through that. I overdid it myself with herbal products. And what that was doing was tearing down my gut even more; it wasn’t rebuilding it back up. And so I just kept in this cycle of herbals and herbals and herbals, but never building. So I no longer do that approach with my patients, unless I find that when I start adding probiotics and for some reason, I can’t get them to adjust to it. They’re still having negative reactions. And I say, okay, they’re fighting each other too much. Let’s come in with a month of Dysbiocide or FC-Cidal, for the SIBO aspect of people. And then we’ll bring in the probiotic. And actually since I made that switch, I haven’t had to really go back to the Dysbiocide or FC-Cidal, I find that the digestive enzymes, the diet that we recommend, which is usually a paleo diet, and then the probiotics on board, I find that bloating goes away, I don’t need to use herbals and everything’s okay.
When it comes to SIFO, I generally like the Fungdx and the grapefruit seed extract along with a binder like Biotoxin Binder. And then when it comes to parasites, I really use a variety of products. Parasites are tricky, they are smart, they like to hide in biofilms. So especially for egg layers, I’ll do a cycle of 10 days with parasitic stuff, usually at bedtime, because that’s when parasites are the most active is at bedtime and you’ll know that because a lot of people grind their teeth at night. They’re jittery, their nervous system is super activated, they twitch. Those are signs of parasitic infections. And so usually a dose at night, 10 days on and then we stop for four days. And the reason why we stop is because that gives time for more eggs to hatch. And then once more eggs hatch, boom, you come at them again. In 10 days, you take another four days off. And we do that for about nine to 12 cycles. So that ends up being about four to five months.
Products I like to use, I use a variety of stuff because I find that once we get one product on, once that product’s done I have to switch to another one and have to switch to another one. Because each of the herbals can target the flukes or the amoebas or the egg layers. So it’s good to just rotate through them all. But I like Wormwood Complex by Mediherb. It is really great. They’re a part of Standard Process. The other one I like is Systemic Formulas. They actually have some great ones, they’re called VRM: VRM1*, VRM2, 3* and 4*. So 1 and 2 are for egg layers. Three, I can’t remember if they’re for amoebas and 4 are for flukes, but they’re going to cover all the types of parasites. So I usually rotate through those. Sometimes I’ll double up and have like a 1 and a 3 on a board. And then a 2 or 4.
My muscle testing, they usually indicate which ones the body wants at that time. And then sometimes I have to put a binder on for my parasite people. A lot of people don’t realize that the fungus and the parasites, they also bind to chemicals. Fungus in particular is a really great heavy metal chelator. So they’re going to bind to aluminum and mercury and cadmium. And so when you start killing these guys, guess what they’re going to start releasing, chemicals and heavy metals and trash. So binders again, the GI Detox is a really great product. I usually do that if I’m having them do the parasitic protocol at night, then I’ll have them do the GI Detox first thing in the morning. As soon as they wake up on an empty stomach, take two of them. I also liked the binder by Systemic Formulas called Bind*. That one’s really great as well.
Lindsey:
Did you ever use the Para 1*, Para 2* (purchase using patient direct code: I0rdLMOm), by CellCore?
Loredana Shapson:
Yep, I do like that. I find that Para 2 only does really well with Para 1 in my muscle testing. So I usually pair those two together. Or Para 2 paired with one of my VRMs. I usually find that of the ingredients in parasitic stuff, like wormwood, clove, artemisia, those are the ones that are really big guns for parasites.
Yeah, well, that’s nice too because it’s got the adrenal stuff in there. So it’s kind of a combo.
Loredana Shapson:
Yeah, I like that, that’s another thing we haven’t talked about is adrenal support through all this.
Lindsey:
Okay, let’s talk about it. What the heck?
Loredana Shapson:
I mean, adrenal support, anything that has to do whenever your body’s under stress, I call the adrenal glands like kicking screaming children, they’re the first ones to fall on the floor and start flailing and going out of whack no matter what you’re going through, so they need support. So I really like ashwagandha and rhodiola as two herbal products that are wonderful for calming the adrenals down.
And then I also really, really like Biotics Research Bio-Glycozyme Forte*. That product is for sugar regulation, but within it, there’s also organ meats like hypothalamus, pituitary, adrenal gland, thyroid; there’s a lot of organ meats in there. And organ meats are paramount in healing; it’s one thing that we lack in our diet. Even if we wanted to get access to these things, it’s hard to find. And if you ask our ancestors, they all ate it, they all prized the organ meats; they ate the brain, they ate the heart, they ate everything. So I find that when you strengthen the organs with organ meats, you’re going to get a better, stronger response, hormonally, and with the adrenals as well. So Bio-Glycozyme Forte, I’d probably say 99% of my patients start on that first at the first visit. And they’re on that one three times a day. Yep. And that’s a wonderful product for blood sugar and adrenals. And then again, ashwagandha and rhodiola are some other ones. I bring in some ginseng too.
Lindsey:
And does that matter to you whether they show signs of adrenal dysfunction? Or that’s just kind of everybody?
Loredana Shapson:
Yeah, everyone’s got blood sugar issues. It’s just our diet and the way that we live our lives being so stressed out, we’re constantly so enzymes and Bio-Glycozyme Forte are my big guns that I always start with.
Lindsey:
I’m not sure that you totally answered the question before in terms of order of operations. So if you find somebody has parasites, if they have fungi, if they have bacteria, is there an order that you address those?
Loredana Shapson:
Yeah, great question. So yeah, I generally always go after parasites and fungus first. In terms of size, when we look at their size, they are the bigger ones that live in the body, and the smaller ones like to hide in the bigger guys. So I’ll usually go after fungus and parasites first or sometimes together. And then I’ll go after the bacteria. And usually once the probiotics come on board, it really balances out the bacteria.
Lindsey:
I mean, there’s a lot of crossover really with herbals of what deals with what, right? Like I mean wormwood addresses bacteria to some extent, too, doesn’t it?
Loredana Shapson:
Yeah, there is crossover with a lot of these, like berberine can do fungus and it can do bacteria. So there is crossover, so you’re going to get benefits on both ends. I find that the ones that work for parasites can also work for fungus. So that’s why you’re going to handle both together anyway.
Lindsey:
Well, that was a lot of really good concrete information. I’m sure people are going to love all the takeaways.
Loredana Shapson:
Yeah, there’s a lot in there.
Lindsey:
And you can find all these products in my Fullscript dispensary.
Loredana Shapson:
Yeah, there is an order for how these things should be added in. I wouldn’t jump on all these things at once. It’s a slow, steady process. That’s what we’re here for. Lindsey and I can help you through when to start what and for how long.
Lindsey:
You can waste a lot of money on supplements trying to figure this out on your own. And I’ve discovered that there is a lot of complexity to this stuff over time and supplements are expensive. And if you take them in the wrong way, they can cause harm or they might not work and then you think okay, I’ve tried that. Unfortunately, then in your head “I’ve tried that” becomes a narrative that you then give to the next person you work with, which puts them at a loss for that thing. Okay, well, if you’ve tried that, and that didn’t work, but you maybe you didn’t try it quite the right way, then I don’t have that tool in my toolbox. Because I think okay, well, they’ve already tried it. So, it is better to get the help of someone. That’s the sad reality of it.
Loredana Shapson:
Absolutely. There’s a lot of individuality here. One final comment on probiotics. A lot of the research is showing peak benefit of probiotic uses at two months and sometimes three months. And there’s some studies showing six months when it comes to eczema and skin to your point with your patient. That study was done in children but still they showed that the longer that they were on at the six month mark, people did better than three months of probiotics. So know that time is a thing. And I find that a lot of people come into my office, “Oh, I tried a probiotic for a couple of weeks and it didn’t work.” And I’m like no, no, you didn’t give it enough time or you were using the wrong one like Saccharomyces boulardii, or you know, one with strep, but I don’t really go to the start.
Lindsey:
So tell me where people can find you. And do you see people who are outside of your area?
Loredana Shapson:
Yeah, I work virtually and in person. I’m in Newtown, Pennsylvania, but I do meetings over Zoom. And for people with bloating, I have a freebie on my website, you can go to my website and get my belly bloating fixer elixir tea, and you drink that every morning and that’s going to start fixing the underlying reason for low digestive enzyme release, part of your bloating problem. So I find that people who start that, their bloating reduces or distension comes down. Some people have lost weight in the first week – two pounds – acid reflux goes away. So really great things using stuff in your kitchen. So get your hands on that recipe for free on my website.
And then I also just released a two-week online gut course, also on my website. And I basically structure everything that I do with my patients and the protocol that I use with my patients in this two week program with education and access to all the supplements that we just talked about today and when to use them and why. And it also gives them direct contact with me, so that’s right on my homepage. It’s called “Bye Bye Bloat: Eliminate Bloat in Two Weeks for Good,” so check that out. I specialize in women so I mean, anyone can really do that program to be honest with you, but women is who I typically work with in my office, and I have a YouTube page. I’ve got free health tips there. You can also find me on my Instagram and Facebook.
And if you’re struggling with bloating, constipation, diarrhea, soft stool, acid reflux, IBS, IBD or any type of chronic disease, etc. and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me (Lindsey). We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
Tell me about what the benefits of fermentation are over probiotics, and what fermentation is.
Holly Howe:
Okay, it’s a great place to start. Let’s start first with fermentation. And the way I like to look at fermentation is that we’re taking vegetables, and we’re transforming them into gold. They become magical foods that improve our gut health. We can’t do it alone; we need the help of bacteria and the microbial world. These vegetables come with bacteria. As the plants are growing, the bacteria nestle on these vegetables, and we set up a home for them through fermentation, packing foods into a jar or crock. These bacteria get in there, they eat the sugars, and they transform them into lactic acid, which is a digestive aid and a preservative. All of a sudden that lowly cabbage has turned into this gold that helps us with digestion, takes care of our gut microbiome, adds probiotics, prebiotics, and all sorts of wonderful nutrients to our diet. It’s through the ingestion of these fermented foods that we can improve our gut microbiome and our overall health.
People think probiotic capsules in a jar that you can buy off the shelf in a grocery store are easy and convenient. You’re popping a pill. It’s that easy. We can get ourselves in trouble with probiotics. It’s a multimillion dollar industry, and we just have to be careful with why we’re taking their probiotics and what they’re for. Probiotics are designed around a few specific species of bacteria that scientists and biologists have thought our bodies need. When we take a probiotic, we’re taking billions of this one singular strain of bacteria. While probiotic foods are full of millions of bacteria, they come as a whole package. When we isolate that one strain, like they are in probiotics, it can wreak havoc in our body and upset the gut microbiome. If you have a specific health issue, and you’re working with a practitioner, then probiotics might be doing some good for you. Recent studies are showing that we’re not so sure of how they can impact our health and our gut microbiome. They can introduce too much of one strain and kill off another strain, or sometimes they just create an imbalance. If you’re dealing with a severe health issue and working with a practitioner, then by all means probiotics will help you through that process. But for us just to go: “Oh, we want to improve our gut health. Let’s go pop these pills.” In reality, food is where it’s at, and food is where we’re going to heal from. We heal by eating traditional foods, and I think it’s very hard to pop a pill and reap the same benefits.
Lindsey:
Plus, there are so many different types of probiotics, and so many different strains. Unless you have a really good source about which strains are good for which conditions, then you are at risk of choosing the absolutely wrong probiotic. For example, if you’re someone who has histamine intolerance or histamine sensitivity, you would not want to take a probiotic that has high histamine producing strains. That would be an example of going wrong with probiotic pills.
Holly Howe:
Exactly. I believe our taste buds have also missed the pleasure of consuming fermented foods, because these foods add a great umami punch. Adding fermented foods also nourishes our meal and makes it so much better, and it becomes more pleasurable. So yes, you have to work with somebody who knows what they’re doing to make sure you’re not upsetting things when using probiotics.
Lindsey:
What is a good place to start with fermented foods?
Holly Howe:
If you are not used to consuming fermented foods at all, it doesn’t hurt to go out and buy some instead of making them. I teach people how to ferment. I love fermentation. I love the process. Traditional healthy cultures all consumed some type of fermented foods, which I was drawn to. This was 20 years ago when there weren’t many different choices of fermented foods available. I started out by buying fermented foods, and while that’s a great place to start to get used to the flavor of it, eventually it gets too expensive. You start wanting to get your hands involved in the process in order to understand it. If you want to buy fermented foods, there’s a lot out there nowadays. There’s kefir, kombucha, sauerkraut, and pickles. You need to be sure when you purchase fermented foods that you’re buying live fermented foods. The benefits of the fermented foods come from the probiotics, but probiotics in fermented foods are killed off at high temperatures. So if you’re walking down an aisle at a grocery and pulling a can of sauerkraut off the shelf, that can is not going to give you the probiotic benefit. You’ll get the benefits of the fiber and the nutrients in there, but in order for that food to be shipped across the country, they heat, process, and can it. This process kills off all the benefits.
When you’re looking for fermented foods to buy, sauerkraut is a readily available option to start with. You want to look in the refrigerated section, and you want to look for something that says live, raw, and unpasteurized. Also be sure to look at the label and check the ingredients. You should just see the vegetables, the cabbage, and salt. That’s about it. When I first started making sauerkraut, I added dill to it. That was the only way I flavored it. Now I have all sorts of wonderful, flavorful ways to enjoy that sauerkraut. So, when buying sauerkraut, you may see other vegetables with the cabbage. Some brands will introduce other bacteria into the fermentation process. When I make it for myself though, I like to include only the vegetables, because they offer us so much good bacteria already. Basically, if you shop for fermented food, just look for salted cabbage and vegetables on the label and check that it’s raw and unpasteurized. That’s a great way to get used to the flavor of fermented food.
Lindsey:
Are there particular brands you like of sauerkraut?
Holly Howe:
I live in Canada, so I’m not familiar with a lot of American brands. I also haven’t bought much in the way of sauerkraut. As long as you’re looking, new companies come out all the time. You can even find it on Amazon. Don’t try to buy something that is difficult to access. Your local farmers market might even sell some sauerkraut, depending on what artisans are there.
Lindsey:
We used to have an amazing stand near Takoma Park, Maryland, which is outside of DC. It sold sauerkraut and kimchi, and included different flavors and different colors of cabbage.
Holly Howe:
When we start buying local like that, we’re supporting our economy. We’re supporting our farmers. We’re working together as a community, just like we need to work with the bacteria on our vegetables as a community in order to get those benefits.
Lindsey:
You mentioned you do all sorts of fancy things with your sauerkraut. I make sauerkraut myself but I never do anything other than just basically salt. Tell me what kind of fancy changes I could do to my sauerkraut.
Holly Howe:
One of my most favorite ones is what I call Hawaiian sauerkraut. That has pineapple in it. It has cilantro and lime juice and lime zest, and a few other spices. It’s a very summery, cooling sauerkraut. You can start pairing your sauerkraut with your meal, depending on what your meal is, just like you would a wine. My teaching recipe on my website uses grated carrots and chopped ginger, which is a nice balance. The color of the carrots adds some nice brightness. When fermenting cabbage by itself, if it is stored for too long, there’s not enough moisture in it. By adding radishes and carrots in, or grated beets, we’re able to add some moisture into it. To succeed with fermentation you need to have enough brine that everything can be packed down below it. Brine is where these bacteria live in an anaerobic environment without air. By adding a few extra vegetables to the cabbage, not only do we get this beautiful flavor, which appeals to many people’s palates, but then we have some extra moisture to help out. Another favorite of mine is grated beets with garlic and cumin seed. It’s just a beautiful color and the nutrients in the beets help with liver detoxification. You can put pretty much anything you want into a sauerkraut recipe.
Lindsey:
I usually just make plain sauerkraut, but there often isn’t enough moisture. So I have gotten in the habit of just making a little bit extra brine with salt, just to cover the sauerkraut up. Once in my entire time making sauerkraut in the last five or seven years, my sauerkraut just smelled off. I had put a folded up piece of the exterior (of the cabbage) on top, folded up, which doesn’t need to be under the brine. I had been less careful about pushing it under the brine every day. Finally, I opened it up and it was moldy, but I thought I’ll just take that off and everything underneath should be fine. The smell was still off, though. I tried a bit, and thought, “Oh no, that’s not right.” I just spit it out, washed my mouth out, and threw it all away.
Holly Howe:
That can happen once in a while. We don’t always know why. I had one batch of sauerkraut that I tossed. It was because I made it from cabbage that had been sitting in my garage for months. I kept saying that I was going to make it tomorrow. Being the thrifty person that I am, I finally got started. These cabbage heads had turned from a dark green to a blonde white. They had no weight to them. There were brown bits that I had to cut off. Don’t ask me why kept going, but I did. I made sauerkraut. We were just raised not to waste food. I made a five liter batch of it and it fermented fine. It looked okay, and I packed it into jars, then put the jars in my refrigerator. I pulled a jar out later to take to a gathering, but when I opened it up, there was a thick layer of pinkish-brown slimy mold on top. There was not enough bacteria in that head of cabbage because it had been in the garage for at least two months. The bacteria couldn’t do the work because there weren’t enough of them. I knew right away that it needed to be tossed. We have to use the best ingredients possible. We’re setting up a good home for the bacteria. They like a certain amount of salt. They like a certain temperature. They’re picky like the rest of us. If we set up the right home for them, it’s failsafe. It’s very hard to ruin a batch. Like you said, intuitively, you knew that batch was wrong. Fermentation is very safe. There’s never been a recorded case of illness for eating fermented vegetables. It’s a very safe process.
Lindsey:
Just make sure it stays under that brine. This last time every day I just made sure I pushed everything under the brine so it all got wet again. Sometimes the veggies do push up out of it. Do you have a device that keeps things under the brine when you ferment?
Holly Howe:
20 years ago, when I first started fermenting, Amazon wasn’t around. The way that we fermented was in large crocks. Today, everybody’s fermenting in jars, which is a great way to learn. It’s also a great way to do all your fermentation. They have come up with neat little devices to create an air seal, and also to hold things under the brine. My favorite device is called a fermentation spring*. I received one in the mail a few years ago from a company called Trellis & Co. A spring engineer developed the technology but it’s a wound spring, a piece of metal in a spiral, that you put into the top of your jar. The lid on your jar forces the spring down, and the spring puts pressure on your packed jar of cabbage. This holds everything under the brine splendidly.
Most of the original fermentation weights for jars were glass disks, because they copied what people used to do in a large crock. Our great-great grandparents, when they fermented sauerkraut in the basement, would pack the vegetables into a large crock and put a large plate on top. Then, on top of the plate, they would put a heavy can, or some type of large weight that pushed down hard on that packed cabbage. They could put a lot of weight inside a large crock. In a little jar, a little glass weight just does not push down hard enough during the fermentation process when all these gases are being created. Those gases push up by creating air pockets which push everything out of the brine. What you’re doing everyday by pushing into the brine works great, or by using my favorite device, a fermentation spring.
Lindsey:
I forgot one other piece to my fermentation mishap. I usually take a clean dish towel and lay it over my jars just to keep sunlight out. That time I took a dirty dish towel to cover the jar that we’d been using to dry our hands with. There was probably a good bit of random bacteria on it.
Holly Howe:
It’s a very forgiving process. Even that dirty towel and some bacteria that may be dropped into the brine, those bacteria are creating a safe environment in the jar for the vegetables. They get rid of the chemicals sprayed on our vegetables during the fermentation process. It’s just amazing what they’re able to do. Who knows what went wrong; you never know.
Lindsey:
I have a little sauerkraut with my egg at breakfast and maybe a coconut yogurt a few days a week. How could I incorporate more fermented foods into my diet?
Holly Howe:
Number one, just realize that you don’t need to eat a lot of the fermented foods. Think of it as a condiment. To me, the easiest way to add fermented foods to your diet is to just add them to a meal like you do with your eggs. When I’m eating dinner, I’ll just put a dollop on the side or when I make a salad at lunch, I’ll sprinkle some of that onto my salad. The easiest way to incorporate sauerkraut is to add it to your plate, but some people don’t like the taste of it. They may not be used to the sour taste. If you did not grow up with fermented foods, the sourness of them can be an uncomfortable flavor to get used to.
You can add it to a salad, so if you’re making a green salad you can add some shredded cabbage to it. You’re not even going to notice the sour flavor. In fact, it’s going to add to the salad; it will taste so much better. It’s just like adding vinegar to your salad. People have been known to take the brine and put it into a smoothie. That will help you get the beneficial bacteria and the probiotics into children who do not want to eat the fermented food. Just add the brine or even the sauerkraut into the blender, blend it up, and it’s a hidden way to sneak it in. You could also try layering it into a sandwich or onto a hamburger. Some people make Buddha bowls with sauerkraut. It’s just one more vegetable to add in.
Fermented carrot sticks are a great way to get children to start eating fermented foods. You can dip them into hummus or ranch dressing or a different dip. There are many ways to mask the flavor of it and then other ways to just let it sit there and be prominent on your plate. In my opinion, sauerkraut tends to add to your meal. Meals taste so much better with fermented foods. You’ll get to a point where every time you start to eat your dinner, you’ll think something’s missing. You’ll go grab a jar of sauerkraut or pickles or fermented carrot sticks. All of a sudden your taste buds are turned on and the food tastes so much better. That’s because of the umami taste in fermented foods, which is a pleasant savory taste. Chefs know the secret of adding umami-rich ingredients to meals because it brings out all the flavors.
Lindsey:
As I mentioned, I eat it with my breakfast. I’ll have a bite of egg with some chipotle hollandaise sauce and a little bit of sautéed spinach and then a little bite of sauerkraut. The sauerkraut adds in the salt component.
Holly Howe:
Yeah, exactly. We have to be careful too. If you’re brand new to fermented foods, sometimes your body likes it so much. It craves it. You start eating that jar of sauerkraut, and you almost want to go to the bottom of it in one day. It’s just like with those probiotic supplements, you don’t want to introduce too much bacteria all at once. You have to be careful with fermented foods not to add too much all at once. You should start very slow. If you have compromised gut health, even just taking a sip of the brine for a few days, and testing how your body reacts to it. If after a bit, you body is doing okay, then maybe sip a little bit more once or twice a day. Work your way up gradually over like even a month. Take it slowly because it’s much easier to back off than it is to undo damage of throwing too much bacteria into your gut too quickly. Work your way up to one or two forkfuls of sauerkraut once or twice a day, and that is plenty to help you with your gut health. Then think about adding other fermented foods to your diet. Kombucha is real popular. Milk kefir is another great one to add to your diet. Also, try fermented pickles, or various fermented vegetables. You’ll get a variety of bacteria introduced into your gut microbiome.
Lindsey:
Do you do your own yogurt or kefir?
Holly Howe:
I do my own milk kefir, on and off. Right now, I’ve switched over to making a special yogurt. That being said, I love milk kefir. It is great for people with compromised gut health, who might be intolerant to dairy. The fermentation process breaks down the lactose and makes it much more digestible. There are more strains of beneficial bacteria in milk kefir than there are in yogurt. It’s a very wonderful food to add into your diet when you’re trying to take care of a lot of gut issues. Milk kefir is made ideally with raw milk, but you can make with any type of milk. The next step is adding what they call milk kefir grains, which look like little pieces of cauliflower. They’re a symbiotic collection of bacteria and yeast. You’re putting that into your jar of milk, and you’re letting it sit on your counter anywhere from 12 to 36 hours. It will thicken and sour and then you drink the milk kefir. It’s a very easy fermentation process. It’s easy to find milk kefir grains on many different Facebook groups. That’s a great way to take care of your gut health.
Lindsey:
Are you not heating the milk at all in the way you do when you make yogurt?
Holly Howe:
No, you don’t heat the milk at all. That’s why it’s so nice, because you have nothing to do other than removing the grains after the fermentation process. I was even doing this with a bare hand because the grains were large enough. I’d just reach into my jar when it was done fermenting, pull the grains out of the jar, and put them into the next jar. If you want to be careful, you should strain them through a strainer. I find the process so simple. No heating at all. You can just keep reusing the grains over and over. They grow and grow. You might even have to donate some to a friend because the grains have gotten too big. When there’s more grains, the fermentation process happens more quickly. Milk kefir is just a wonderful drink. Some people do make it with coconut milk. If you are sensitive to dairy, it’s worth a try, because many people find they can digest it without any issue at all. It has so many good healing properties.
Lindsey:
I’ve made yogurt; I used to make a wonderful lemon yogurt, which was something I tried for the first time when I was studying abroad in France. I would also add rosewater sometimes. There were seven jars that fit into the yogurt maker and I would add a little bit of whatever flavoring, so I could have multiple flavors in one batch. That was when I was eating dairy. I’m very picky about coconut yogurt. There’s literally only one brand I like, which is called Cocojune*. That’s the only one I eat. I haven’t tried ever to make kefir myself with non-dairy milk.
Holly Howe:
Right. I haven’t played with non-dairy milks, because I personally just want the nutrition out of the dairy, and I’m good with dairy. One thing I’ve gotten on to recently is Dr. William Davis, who wrote the “Wheat Belly*” book. He’s been experimenting around making yogurts with specific strains that he calls keystone species. These are species of bacteria that we should all have in our diet. He’s finding that people are lacking in them. This book called “Super Gut*” teaches you how to make yogurt from these different strains of bacteria. The one I’m making right now is called L. reuteri. You use capsules that have the L. reuteri species strain in them, and you make it with pasteurized milk, not with raw milk. The idea is that you only want to introduce the strain that he’s trying to reinnoculate into your gut microbiome. You don’t want it to compete with the other strains that could be found in the milk. You make this yogurt at a specific temperature – 100 degrees – and you do it for 36 hours. It has tremendous gut healing properties, and it’s also skin smoothing, and makes you sleep better. It becomes a miracle yogurt when you work with a specific strain that makes all sorts of wonderful things happen.
Lindsey:
My understanding is that a traditional yogurt-maker is at a higher temperature than what he uses. You have to use something special, like an Instapot. I understand that the newer ones will keep things at a particular temperature like 100 degrees.
Holly Howe:
Exactly, you have to be able to control the temperature. With the newer instant pots, you can easily control the temperature. There are also specific yogurt-makers that allow you to have control over the temperature. You can also use a sous vide cooker. I make my yogurt with a sous vide cooker and a big pot of water with three or four jars of yogurt in there.
Lindsey:
So like you put a wand in and the sous vide cooker keeps it at a certain temperature?
Holly Howe:
Yes. That works well, because I already have lots of jars in my house. I don’t really use drinking glasses. Instead we drink everything out of various canning jars, so we have these jars in all sizes. I just didn’t want to introduce a new set of jars into the house with the yogurt makers that have those nice cute little jars. I found that by using the sous vide wand in a spaghetti pot of water, I could put three jars in the pot and make a two to three liter batch of yogurt all at once. That tends to work well in our family.
Lindsey:
Has it been giving you those amazing benefits?
Holly Howe:
I’m noticing a great difference in sleep, and I’m also noticing that my dreams are much more vivid. I didn’t used to remember dreams at all, and now I’m remembering my dreams. I ran into a girl in the market the other day who was getting ready to make another batch of her yogurt. She said, “Look at me! I’m seventy, and I have no wrinkles.” It’s just wonderful.
Lindsey:
That’s it. I’m making it–you’ve convinced me. Anything for vanity! Are there ferments that you particularly like for people with gut health issues?
Holly Howe:
Definitely make the milk kefir. I’d also recommend starting with what I would call “gut shots” or the juice from the sauerkraut. You, in essence, make a watery batch of sauerkraut and you drink just the brine from it. A lot of times people with gut issues cannot take the fiber from the sauerkraut, so I think gut shots are a wonderful way to gently introduce the beneficial bacteria without actually consuming the fermented food. Bone broth would be another option that is so healthy and healing for people with gut issues.
Lindsey:
I love my bone broth. During the winter, I try and have that every morning with some lemon and salt in it.
Holly Howe:
Yeah, exactly, it’s so nourishing and so healing. There are just so many things we can do to take care of our health through foods that for traditional cultures, it was their mainstay diet. People should really stay away from processed foods and go back to these original foods. It can be so healing for the gut.
Lindsey:
I think of fermentation as sort of an accidental thing. Back then, they probably needed to preserve the food, so it fermented and then that’s how it stayed good.
Holly Howe:
Exactly. Fermentation is not just a recipe you want to try for the day, where you open up your cookbook, as if you want to make a batch of chocolate chip cookies, and you run to the store and buy everything. Fermentation is actually a way to preserve foods. If we’re going to have success with fermentation, we need to preserve what is locally available and in season. If it’s December and I want to make pickles, just like I’d want to make chocolate chip cookies in December, I’m going to be fighting with the ingrediants. I’m not going to have much success because the cucumbers sold in December were either grown in a hot house, or they were shipped from halfway around the world, or they’ve been sitting on the shelf for weeks. We have to reflect on what is the number one worker bee that makes fermentation happen: it’s the bacteria. The minute that we pick a vegetable that we want to ferment, it’s trying to decay. The bacteria that break it down are fighting with the bacteria that are going to transform it into gold for us. We really have to look at fermentation as a way to preserve foods, and we should be preserving our local foods. When we work with something local, that was recently picked, it’s very hard to mess it up, because it’s just teeming with that beneficial bacteria.
Lindsey:
What are some of the more advanced ferments that people might consider making if they’ve already done the basics, like sauerkraut or yogurt?
Holly Howe:
Well, like I mentioned before, fermenting cucumbers into pickles is one of the more advanced ones in my opinion. It’s just a little more finicky. If you’re starting with fresh-picked cucumbers, it’s hard not to mess it up. Sometimes they come out too soft because you haven’t added enough tannin-rich vegetables in there. You have to cut off the blossom so the veggies don’t soften during the fermentation process. Also, people pick fresh cucumbers in the middle of summer, which means we’re fermenting in the heat. Ideally, fermenting works better at cooler temperatures, which is difficult when your house is 80 degrees. Often, if you want to make your fresh, local cucumber pickles, you’re fighting the heat. The bacteria that help make fermentation happen don’t like the heat. There’s a lot of factors at play when you’re trying to make your cucumber pickles. I ferment them in ice chests where I’ve put a frozen jug of water so I can drop the temperature down. Ideally, you should aim for about 65 to 70 degrees Fahrenheit for your fermentation temperature. When the temperature gets above that, you’re fighting all these other things going on, and your chances for success are greatly diminished. To me, that is a more challenging one.
Kimchi is beautiful to make, but there are just more steps involved. If you’re making it in the traditional format, you’re soaking the napa cabbage in the salt and water first, and then you have to make the paste that the leaves get layered into. That one’s a little bit more complex, but you can get the same flavors by making a kimchi-style sauerkraut, which I have a recipe for on my website. You slice the cabbage up finely and then add green onions and carrots and Korean red pepper and fish sauce to get the same flavors, but in a much more simple process. It’s a learning process, and once you learn the fermentation process, then it becomes intuitive and second nature. You start going to the market and you see everything down there and you can’t stop thinking: “What can I make with that? What can I make with that?”
Lindsey:
My husband grew up near a Korean family in Florida, and he said that they would bury the kimchi in their yard, then dig it out when it was done fermenting.
Holly Howe:
Right. They were burying it in their yard to have that nice cool temperature, that stable temperature. Your best flavors happen when you have a nice stable temperature during the fermentation process.
Lindsey:
Tell me about your fermentation courses and your book.
Holly Howe:
On my website I give people three entry points. I have a great teaching recipe on there. If you want to just jump in and learn how to make sauerkraut, it takes you through step by step. And then in my book called “Fermentation Made Easy! Mouthwatering Sauerkraut,” the book is available on Amazon as a print book or on the Kindle, or on my website as a PDF, it includes 20+ recipes with all my beautiful combinations of flavor. I have The Firecracker Sauerkraut which has sliced jalapenos, oregano and red onion in it. There’s the beet sauerkraut in there. There’s a kimchi sauerkraut in there. I teach the process step by step and you get the recommended tools for how to make various flavors of sauerkraut. I have a course on how to make sauerkraut, and then an online course on how to make fermented vegetable pickles.
Any final thoughts about fermentation for us before we head out?
Holly Howe:
Just jump in and try it! It’s an amazing process. I love it because it introduces people to a whole new community: the microbial community. When I first made sauerkraut, I was following a recipe just like it was a chocolate chip cookie recipe. I did not realize that there was bacteria in there that were making all this magic happen. Once you realize that, it’s just a whole new world, and you start wanting to take care of the bacteria and make sure that you’ve fed them properly and set up their home properly. Before you know it, you’re trying to get the best cabbage possible, so you’re looking for a local community farmers’ market where you can buy great cabbage from your farmer, if you’re not growing it in your backyard. All of a sudden, you’ll sit down at night for a meal and you’ll realize how much of your food came from your local community.
Lindsey:
It is also so much less expensive to make your own ferments. I think you could buy fancy sauerkraut for 10 dollars a jar, and you can make three jars of it from one head of cabbage.
Holly Howe:
Right? It’s more like $20 a jar.
Lindsey:
Oh yeah and it’s like $2.50 for a head of cabbage.
Holly Howe:
We need those skills of fermentation. It’s a very empowering process, when you can slice up this cabbage, and sprinkle some salt on it and pack it into a jar. Then you watch the bubbles happening, and over time you watch the colors change, and the smells change. Eventually, you open up the jar and, all of a sudden, you have something that you made yourself, something that’s going to take care of your gut health. It’s much simpler than a new diet or a new thing you have to do. Rather you just open up that jar and put a fork of the sauerkraut onto your plate, and the meal tastes better, you sleep better, and your gut is healthier. In that way, it’s such a wonderful empowering process. It’s just great to learn a new skill and add it to your repertoire.
Lindsey:
Well, thank you so much for coming on and sharing with us about fermentation. You’re actually the first person I’ve had on the podcast who’s talked about this topic. Take care and thank you so much.
If you’re struggling with bloating, constipation, diarrhea, soft stool, acid reflux, IBS, IBD or any type of chronic disease, etc. and want to get to the bottom of it, that’s what I help my clients with. You’re welcome to set up a free, 30-minute breakthrough session with me (Lindsey). We’ll talk about what you’ve been going through and I’ll tell you about my 3- and 5- appointment health coaching programs in which I recommend lab tests, educate you on what the results mean and the protocols used by doctors to fix the problems revealed. Or if you’re ready to jump in right away or can just afford one appointment at a time, you can set up an 1-hour consultation with me.
Sign up for my Substack newsletter and get my free ebooklet: “Finding Your Root Cause Through Stool and Organic Acids Testing”: